
Navigating Non-Invasive Prenatal Screening: Your Guide to NIPT
Understanding Non Invasive Prenatal Screening Tests
Navigating Non-Invasive Prenatal Screening: Your Guide to NIPT
Follow us here:



During the menopause transition estrogen levels fall sharply, removing a key vasodilatory and lipid‑modulating hormone that helped keep arteries flexible. This hormonal shift accelerates LDL‑cholesterol rise, HDL‑function decline, visceral fat gain, and arterial stiffening, which together raise the prevalence of coronary heart disease, hypertension, and stroke in the years after the final menstrual period. Because these changes can occur before symptoms appear, clinicians recommend proactive screening—annual blood pressure checks, fasting lipid panels, glucose testing, and waist‑circumference measurements—starting in perimenopause. Coupled with evidence‑based lifestyle interventions such as a Mediterranean‑style diet, at least 150 minutes of moderate‑intensity aerobic activity weekly, weight management, smoking cessation, and stress‑reduction techniques, a menopause‑focused heart plan can blunt risk‑factor progression and protect women’s cardiovascular health for decades to come.
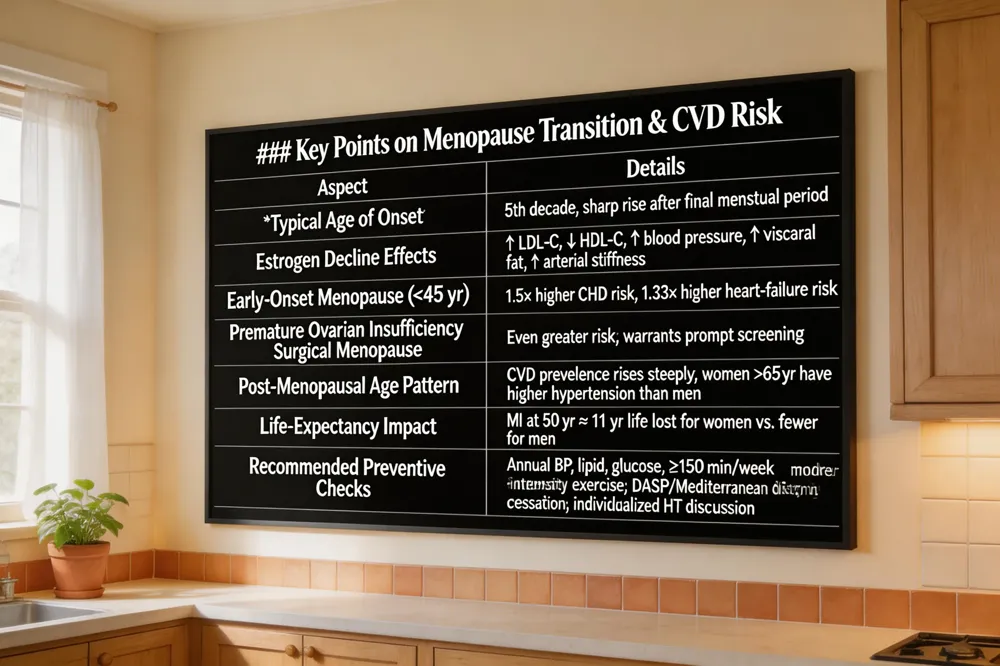 The menopause transition (MT) is a pivotal window when women’s cardiovascular disease (CVD) risk accelerates, usually beginning in the fifth decade and rising sharply after the final menstrual period. Declining estrogen drives adverse changes – LDL‑C rises, HDL‑C falls, blood pressure climbs, visceral fat accumulates, and arterial stiffness increases – all of which promote atherosclerosis. Hot flashes, sleep disturbances, and depressive symptoms further signal heightened risk.
Early‑onset menopause (before age 45) amplifies this danger; studies show a 1.5‑fold higher risk of coronary heart disease and a 1.33‑fold higher risk of heart failure compared with later menopause. Women experiencing premature ovarian insufficiency or surgical menopause face even greater risk and should be screened promptly.
Age‑related patterns reveal a steep rise in CVD after menopause, with women over 65 showing higher hypertension prevalence than men. Because women outlive men, heart disease narrows the longevity gap; a myocardial infarction at age 50 can cost women ~11 years of life versus fewer years for men.
Timely prevention—annual blood‑pressure, lipid, glucose checks (screening of blood pressure, lipid, glucose levels is essential because menopause can elevate blood pressure and cholesterol); ≥150 min/week moderate‑intensity exercise (The American Heart Association recommends at least 150 minutes of moderate‑intensity aerobic activity per week); a DASH‑ or Mediterranean‑style diet (American Mediterranean‑style diet rich in fruits, vegetables, whole grains, legumes, nuts, seeds, and oily fish); smoking cessation (Smoking cessation dramatically reduces cardiovascular risk); and individualized hormone‑therapy discussions (Menopausal hormone therapy (MHT) started before age 60 or within 10 years of menopause may reduce coronary heart disease risk—can blunt risk acceleration and preserve life expectancy.
Estrogen’s Protective Mechanisms
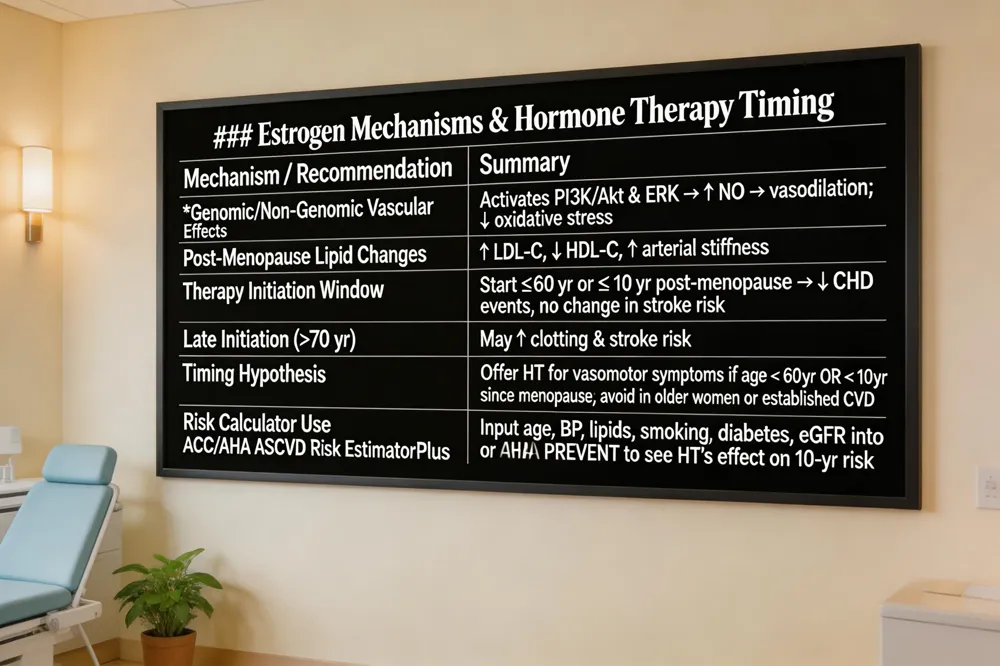
Estrogen supports vascular health through genomic and non‑genomic pathways that activate PI3K/Akt and ERK signaling, boost nitric‑oxide‑mediated vasodilation, and lower oxidative stress. These actions keep LDL‑C low, HDL‑C functional, and arterial walls flexible, reducing atherosclerosis and stiffness. After menopause, the loss of estrogen correlates with higher blood pressure, visceral fat, and a surge in heart‑disease events.
Post‑Menopausal Estrogen Therapy Outcomes
Observational data show that women who start estrogen before age 60 or within 10 years of menopause experience fewer coronary events and lower cardiovascular mortality, while stroke risk remains unchanged. Randomized trials confirm a time‑dependent benefit; initiating therapy after age 70 may increase risk of clotting and stroke.
Menopausal Hormone Therapy Timing
The timing hypothesis guides clinicians: offer hormone therapy for vasomotor symptom relief in women < 60 years or < 10 years post‑menopause, and avoid it in older women or those with established CVD. Individual risk assessment and short‑term use are essential.
HRT Cardiovascular Risk Calculator
Clinicians can input age, blood pressure, lipids, smoking status, diabetes, and eGFR into the ACC/AHA ASCVD Risk Estimator Plus or AHA PREVENT calculator. The tool shows how HRT may shift 10‑year risk, facilitating shared decision‑making and personalized prevention planning.
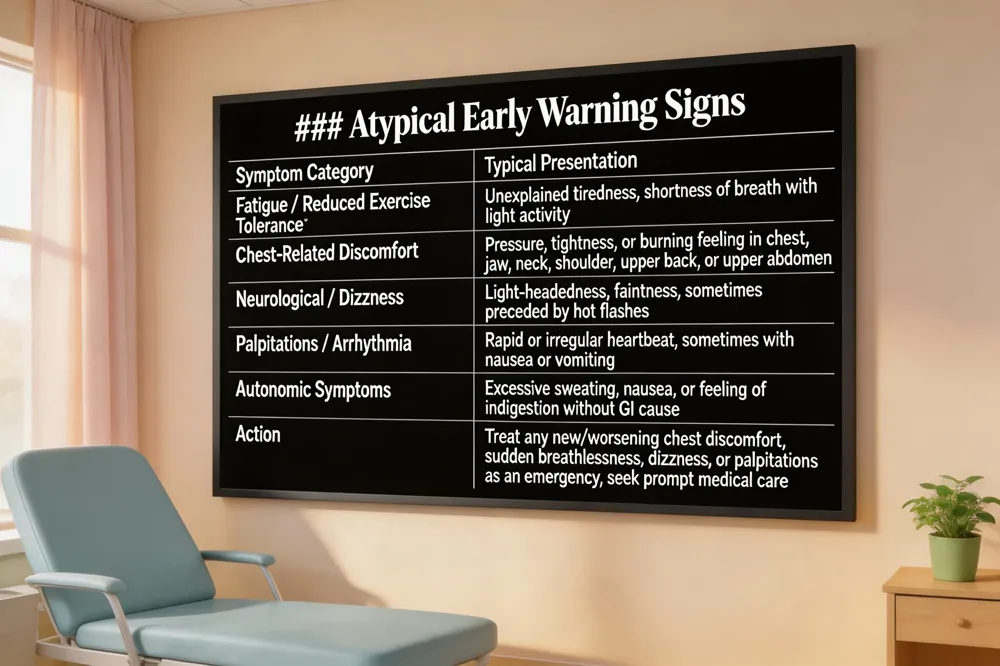 Heart disease often presents differently in women, especially during the menopause transition. Rather than the classic crushing chest pain, many women notice atypical warning signs such as unexplained fatigue, shortness of breath with light activity, dizziness, or a feeling of light‑headedness. Discomfort may appear in the jaw, neck, shoulder, upper back, or upper abdomen and can feel like indigestion or heartburn. Nausea, vomiting, excessive sweating, or a rapid, irregular heartbeat may also signal a cardiac event.
During menopause, estrogen’s protective effect on blood vessels wanes, leading to higher LDL cholesterol, higher blood pressure, and increased abdominal fat—all of which raise heart‑attack risk. Consequently, traditional symptoms (chest pressure, shortness of breath, pain radiating to the arm, neck, or jaw) can be masked by hot flashes, night sweats, or fatigue. Women should treat any new or worsening chest discomfort, sudden breathlessness, light‑headedness, or palpitations as an emergency and seek prompt medical care.
In perimenopause, estrogen decline begins years before the final period, causing lipid changes, insulin resistance, and central weight gain that accelerate atherosclerosis. Regular monitoring of blood pressure, lipid panels, and glucose—combined with a heart‑healthy diet, at least 150 minutes of moderate‑intensity aerobic activity weekly, and individualized hormone‑therapy discussions—helps detect problems early and lower long‑term cardiovascular risk.
Heart‑healthy diet for women
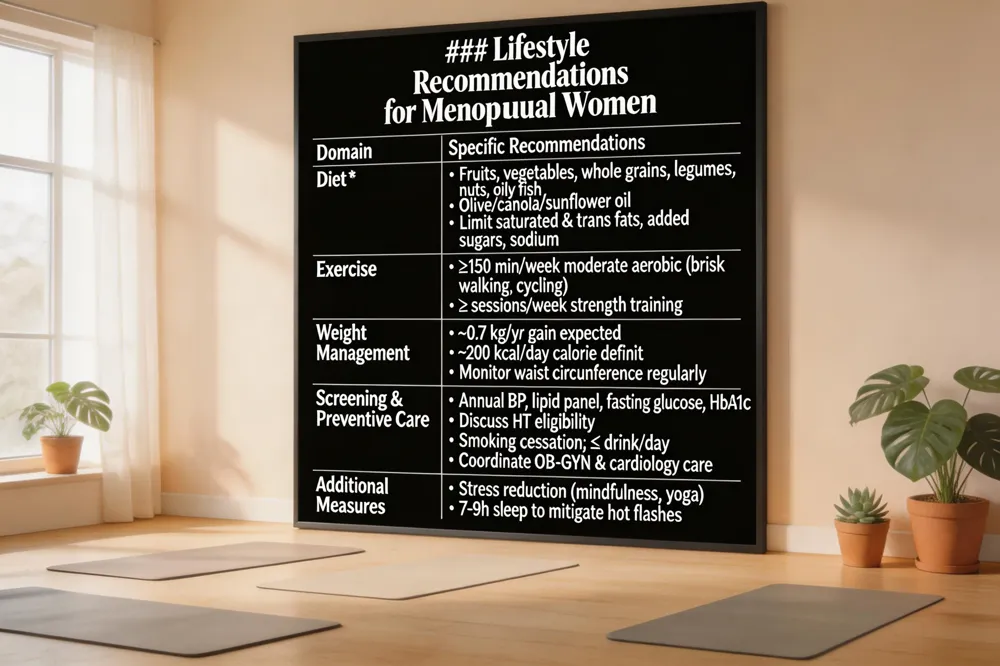
Choose nutrient‑dense foods in appropriate portions: fresh fruits, colorful vegetables, whole‑grain breads, quinoa or brown rice, and lean proteins such as fish, skinless poultry, legumes, nuts and low‑fat dairy. Use olive, canola, or sunflower oil, limit saturated and trans fats, added sugars, and sodium. Pair this eating plan with at least 150 minutes of moderate‑intensity exercise weekly to support weight control and cardiovascular wellness.
Metabolic changes during menopause and their impact on weight management
Estrogen decline reduces lean muscle mass and increases visceral fat, slowing basal metabolism. Women often gain ~0.7 kg per year, especially around the waist, raising heart‑disease risk. Counteract this by creating a modest calorie deficit (~200 kcal/day) and adding strength‑training to preserve muscle, while maintaining an aerobic routine.
Treatment options for heart disease in women
Begin with lifestyle changes—smoking cessation, diet, activity, stress control. Medications (statins, ACE inhibitors, beta‑blockers, antiplatelets) address cholesterol, blood pressure, and clot risk. When needed, minimally invasive angioplasty with stents or coronary artery bypass grafting are considered. Cardiac rehabilitation and personalized follow‑up improve outcomes.
Prevention of heart disease in women
Regular screening for blood pressure, cholesterol, glucose, and waist circumference after menopause enables early intervention. Limit alcohol to ≤1 drink/day, stay physically active, and seek coordinated care between OB‑GYN and cardiology.
Women's heart health facts
Heart disease kills 1 in 3 women in the U.S.; 44 % are unaware. Hypertension affects ~46 % of women, especially Black women. Lifestyle choices—exercise, diet, weight management—can prevent most events.
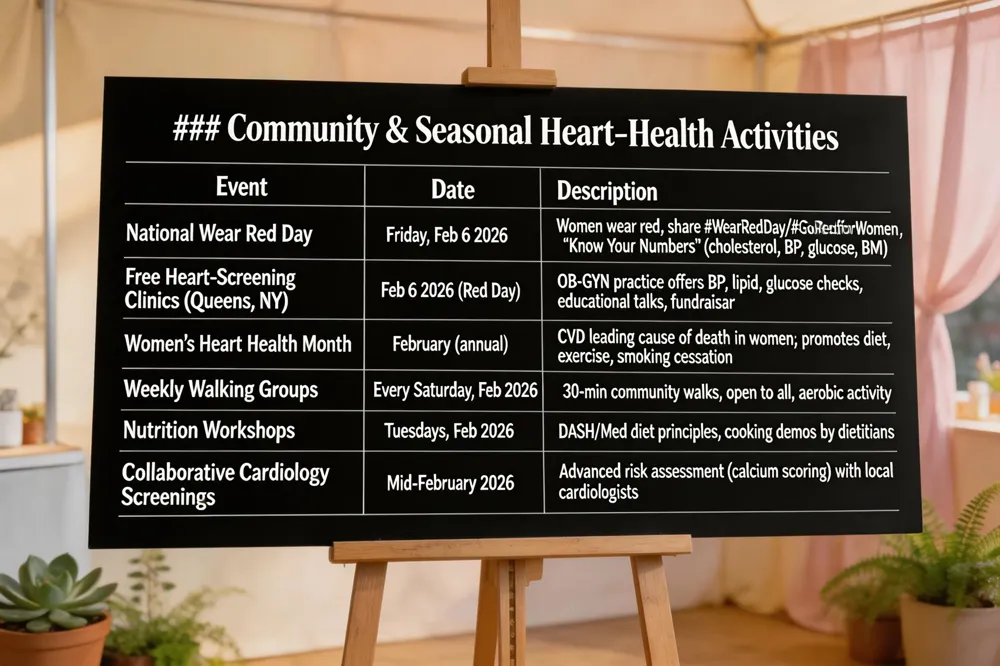 National Wear Red Day 2026 falls on Friday, February 6 and marks Women’s Heart Health Day. The American Heart Association’s Go Red for Women campaign encourages women to wear red, share #WearRedDay and #GoRedforWomen on social media, and "Know Your Numbers"—cholesterol, blood pressure, blood sugar, and BMI—by visiting a health‑care provider. In Queens, NY, our women‑led obstetrics and gynecology practice will host free heart‑screening clinics, educational workshops, and a fundraiser on that day, giving the community a tangible way to participate.
Women’s Heart Health Month, observed each February, shines a spotlight on cardiovascular disease as the leading cause of death for women. It highlights unique risk factors, atypical symptoms, and preventive actions such as a heart‑healthy diet, regular aerobic activity, strength training, stress management, and Smoking cessation. Local initiatives include weekly walking groups, nutrition talks, and collaborative screenings with cardiology partners. By joining these events, women can empower themselves, receive personalized risk assessments, and contribute to research that shapes future heart‑health strategies.
A personalized care plan is the cornerstone of heart‑healthy menopause management. Begin by reviewing your unique risk profile—age at menopause, family history, blood pressure, lipids, glucose, and waist circumference—and set individualized goals for weight, activity, and nutrition. Schedule regular monitoring: at least annually for cholesterol, blood pressure, fasting glucose, and, when appropriate, coronary artery calcium or carotid imaging to catch subclinical changes early. Integrate lifestyle and medical options by pairing evidence‑based interventions—150 minutes of moderate‑intensity aerobic exercise, a DASH‑ or Mediterranean‑style diet rich in fruits, vegetables, whole grains, and healthy fats, smoking cessation, and stress‑reduction techniques—with tailored pharmacotherapy. When symptoms or risk warrant, discuss timely initiation of menopausal hormone therapy (preferably low‑dose transdermal estradiol) or statins, always weighing benefits against potential risks. This collaborative, patient‑centered approach empowers you to protect your heart throughout and post‑menopausal years.
.png)
Compassionate care for every stage of womanhood. Visit one of our convenient locations or book your appointment online today.

