
Understanding Endometriosis: A Guide to Early Detection and Care
Recognizing Early Symptoms of Endometriosis
Understanding Endometriosis: A Guide to Early Detection and Care
Follow us here:



Age is the single most powerful predictor of a woman’s ovarian reserve. After the mid‑30s, the number and quality of eggs decline rapidly, and after age 40 the chance of a natural conception per cycle falls below 10 %. Early identification of this decline allows clinicians to tailor treatment—whether that means using ovulation‑inducing medication, pursuing in‑vitro fertilization, or discussing fertility preservation options—while the remaining egg supply is still robust.
Common early warning signs that should prompt a fertility work‑up include irregular or absent menstrual cycles (oligomenorrhea or amenorrhea), painful periods or chronic pelvic pain (suggesting endometriosis or fibroids), heavy or unpredictable bleeding, and a history of recurrent miscarriage, pelvic inflammatory disease, or sexually transmitted infections that can damage the fallopian tubes. Lifestyle red flags—significant weight change, smoking, excessive alcohol, or high stress—can also signal ovulatory dysfunction.
Timely evaluation shortens the time to diagnosis, reduces emotional distress, and improves the odds of successful pregnancy by allowing earlier intervention, personalized therapy, and, when needed, prompt referral to a reproductive specialist.
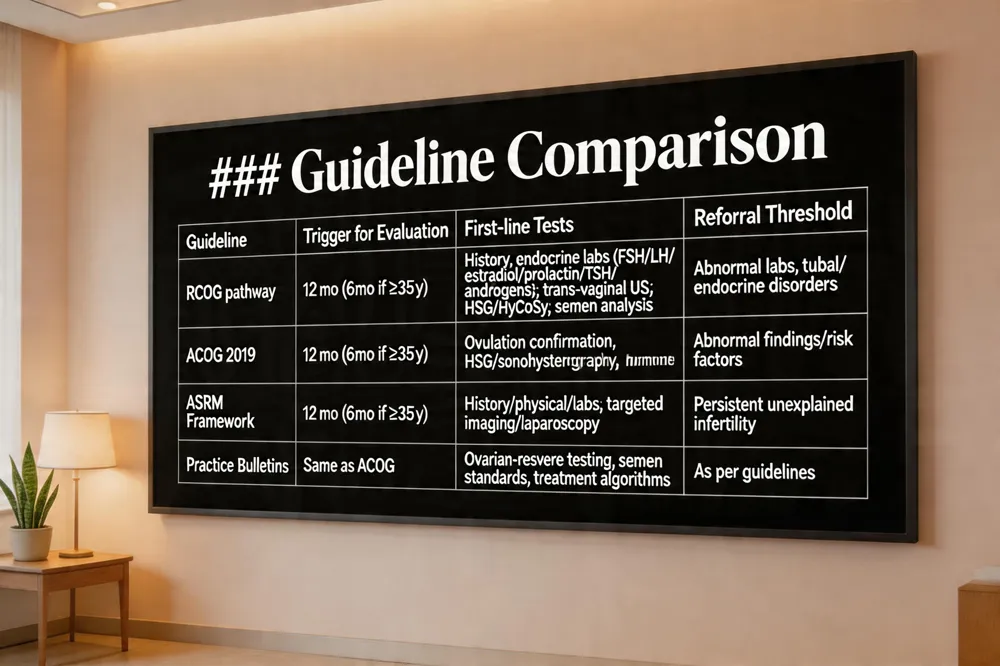 When a couple in Queens, NY, or elsewhere seeks help after a year of trying (six months if the woman is ≥ 35 years), clinicians turn to four cornerstone guidelines that shape a patient‑centered work‑up.
RCOG systematic assessment pathway – The Royal College of Obstetricians and Gynaecologists recommends starting with a thorough history, physical exam, and baseline endocrine labs (FSH, LH, estradiol, prolactin, TSH, androgens). Trans‑vaginal ultrasound evaluates ovarian reserve and uterine anatomy; tubal patency is tested with hysterosalpingography, HyCoSy, or saline‑infusion sonohysterography. Male semen analysis is performed simultaneously. The guideline stresses multidisciplinary referral, diagnosis by exclusion, and early lifestyle counseling.
ACOG work‑up timing and recommendations – ACOG advises initiating evaluation after 12 months of unprotected intercourse (or 6 months when ≥ 35 years). First‑line tests include ovulation confirmation (mid‑luteal progesterone or LH surge), hysterosalpingogram or sonohysterography, and basic hormone panels. Prompt referral to a reproductive endocrinologist or urologist is encouraged when abnormal findings arise.
ASRM best‑practice framework – ASRM defines infertility similarly and promotes a cost‑effective, stepwise approach: detailed history, physical, basic labs, then targeted imaging or laparoscopy for women with irregular cycles, known tubal disease, or risk factors. The society also offers committee opinions on fertility preservation and equitable access for marginalized groups.
Practice bulletin and PDF resources – ACOG’s Practice Bulletin (latest update 2019) and its downloadable PDF provide clinicians with tables on ovarian‑reserve testing, semen analysis standards, and treatment algorithms, ensuring that care remains evidence‑based, compassionate, and aligned with the latest women’s health standards.
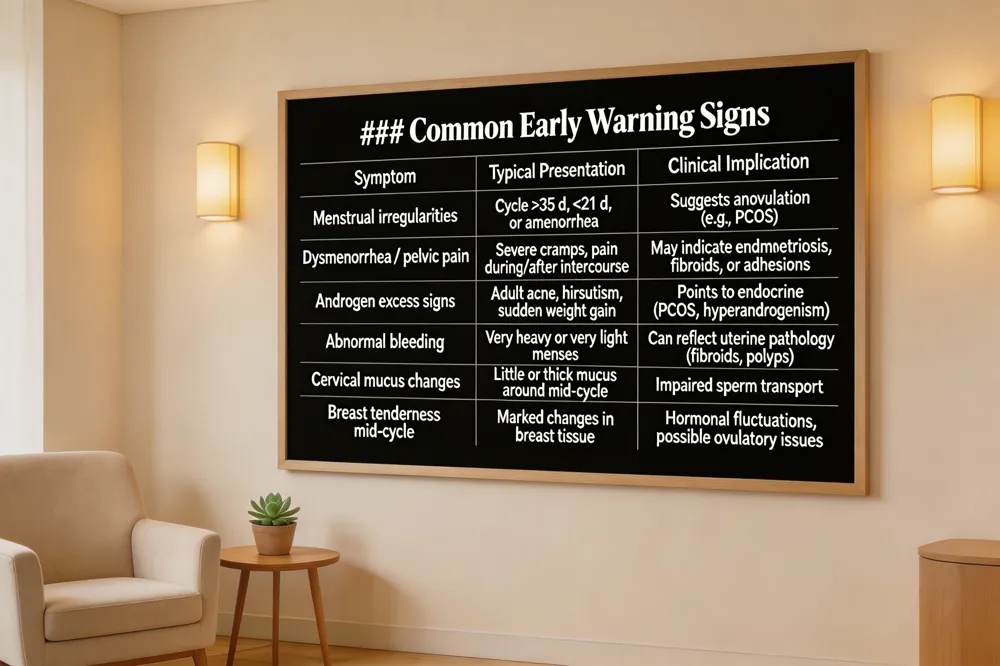 Early signs of female infertility often appear as menstrual irregularities. Cycles that are consistently longer than 35 days, shorter than 21 days, or completely absent suggest anovulation and should prompt a conversation with a clinician. Painful periods, severe dysmenorrhea, or chronic pelvic discomfort—especially during or after intercourse—can signal endometriosis, fibroids, or tubal adhesions that interfere with conception. Hormonal skin changes such as adult acne, hirsutism, or sudden weight fluctuations point to endocrine disorders like PCOS, another common cause of ovulatory dysfunction.
In adolescents, these clues may emerge early: irregular or missed periods, persistent pelvic pain, and signs of excess androgen (acne, facial hair) warrant evaluation even before a desire for pregnancy. For any woman, the most obvious red flag is failing to become pregnant after one year of regular, unprotected intercourse (six months if over 35). Other early warnings include unusually heavy or light bleeding, recurrent ovarian cysts, and changes in cervical mucus or breast tenderness around mid‑cycle.
If any of these symptoms are present, seek a fertility work‑up promptly. A basic evaluation includes a detailed menstrual history, hormone panels, trans‑vaginal ultrasound and possibly a hysterosalpingogram to assess tubal patency. Early detection enables timely treatment—whether lifestyle modification, medication, or assisted reproductive technology—improving the chances of a successful pregnancy.
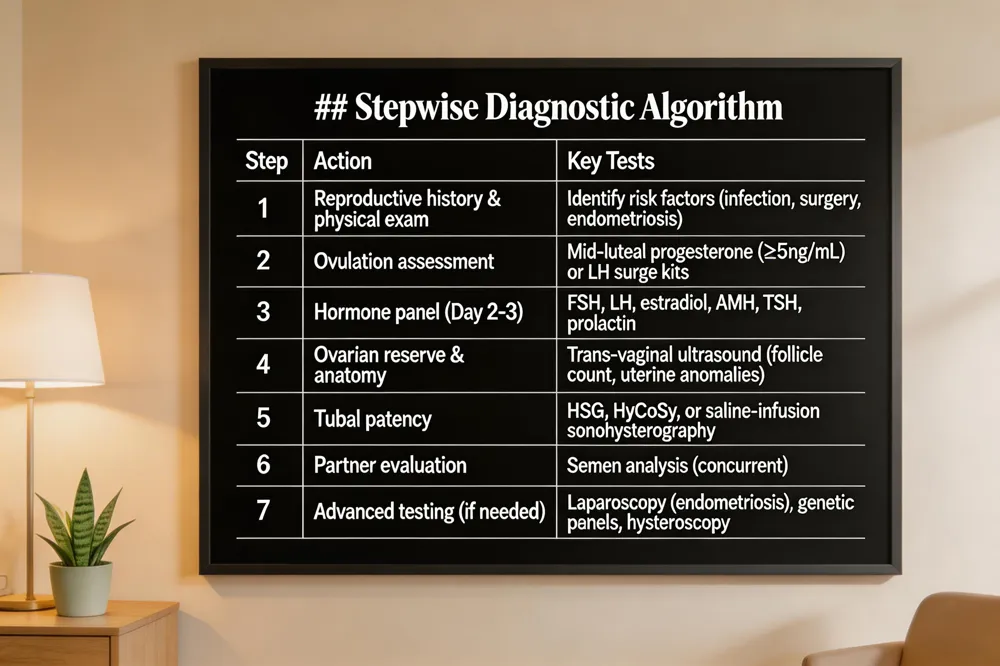 Infertility workup for women begins after 12 months of regular, unprotected intercourse (6 months if 35 y). A detailed reproductive history and focused physical exam identify risk factors such as irregular cycles, prior pelvic infection, endometriosis, or uterine abnormalities.
How to test if a woman is infertile – Blood work assesses ovulation (mid‑luteal progesterone) and hormone panels (FSH, LH, estradiol, AMH, TSH, prolactin). Transvaginal ultrasound evaluates ovarian reserve and uterine anatomy; hysterosalpingography (HSG) or hysteroscopy checks tubal patency when indicated.
Infertility workup labs – Day‑21 progesterone confirms ovulation. Early‑cycle (day 2‑3) labs include FSH, LH, estradiol, TSH, and prolactin.
Infertility workup meaning – The systematic evaluation determines why conception has not occurred, guiding personalized treatment from lifestyle changes to assisted reproductive technologies.
Female infertility workup algorithm – Start with history, exam, ovulation confirmation, and ovarian reserve testing. If ovulation is normal, assess uterine cavity (ultrasound) and tubal patency (HSG). Advanced testing (laparoscopy, genetic panels) is reserved for unexplained cases.
Female infertility guidelines – Follow ASRM and WHO recommendations: prompt evaluation for women ≥ 35 y or with risk factors, prioritize minimally invasive tests, counsel on weight, smoking, alcohol, and stress, and coordinate care with the male partner for a comprehensive, patient‑centered approach.
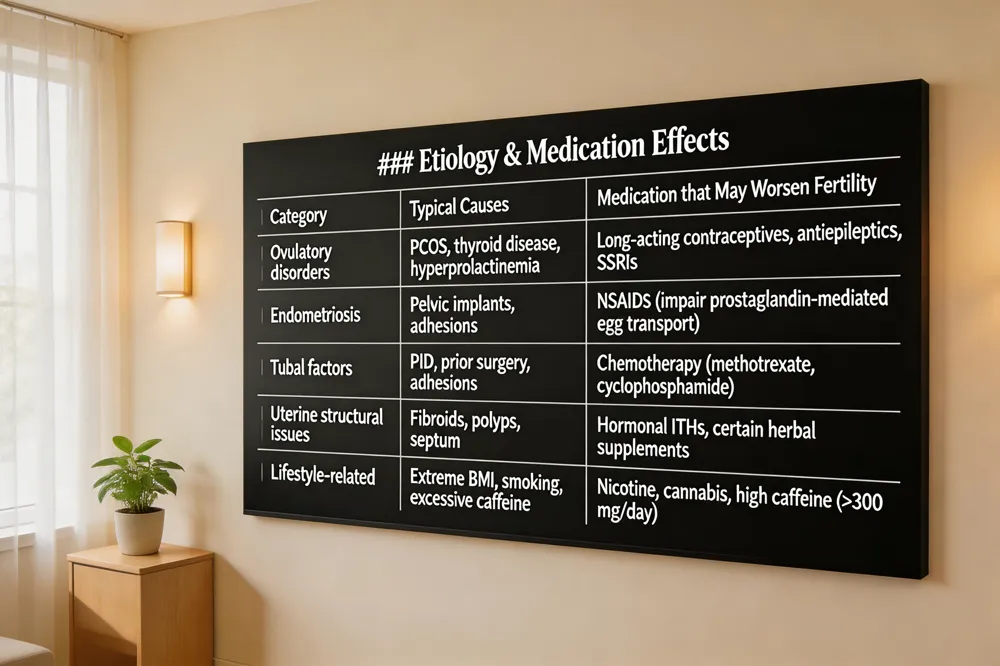 Infertility most often arises from four key categories. First, ovulatory disorders—particularly PCOS—disrupt the regular release of a mature egg, leading to irregular or absent periods. Second, Endometriosis and resulting pelvic adhesions can scar fallopian tubes and impair implantation. Third, tubal blockage from prior pelvic inflammatory disease, infections, or surgeries prevents sperm‑egg interaction. Fourth, uterine structural issues such as fibroids, polyps, or congenital malformations hinder embryo implantation.
Certain medications can further diminish fertility. Chemotherapy agents (e.g., methotrexate, cyclophosphamide) damage ovarian reserve, while long‑acting hormonal contraceptives suppress ovulation and the uterine lining. Non‑steroidal anti‑inflammatory drugs may interfere with prostaglandin‑mediated egg transport, and some antiepileptics or antidepressants are linked to menstrual irregularities. Even over‑the‑counter substances—excessive caffeine, nicotine, cannabis, or herbal supplements—can affect hormone balance.
A diagnosis of infertility does not preclude pregnancy. Many women conceive naturally, especially if the cause is mild. When needed, treatments such as ovulation‑inducing drugs, IUI, IVF, or donor‑egg programs can substantially improve success rates. Prompt evaluation by a reproductive specialist, particularly for women over 35 or with red‑flag symptoms, offers the best chance for a healthy pregnancy.
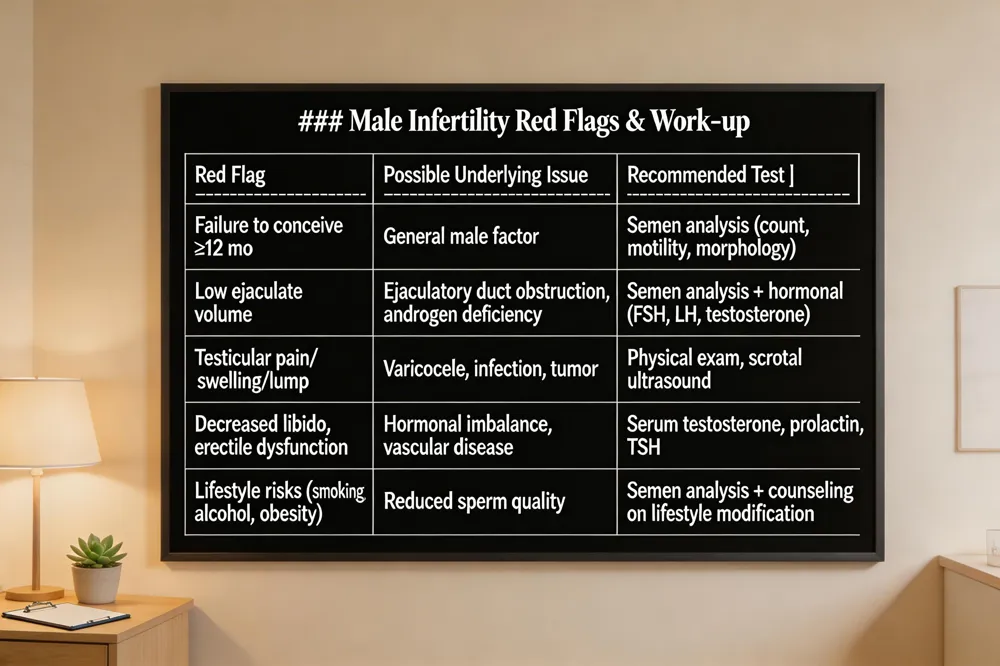 Understanding the male contribution to infertility is essential for any couple trying to conceive. The most frequent signs of male infertility include a failure to achieve pregnancy after a year of regular, unprotected intercourse, reduced libido, erectile dysfunction, low ejaculate volume, or pain, swelling, or a lump in the testicles—often due to a varicocele. Hormonal clues such as loss of facial or body hair, decreased muscle mass, persistent fatigue, or unexplained weight gain may signal low testosterone affecting sperm production.
If you notice any of these symptoms, a semen analysis should be pursued promptly. This laboratory test evaluates sperm count, motility, and morphology and is the definitive way to confirm male factor infertility. The analysis is typically performed after 48‑72 hours of abstinence and provides a clear picture of reproductive potential.
Male health directly impacts a couple’s fertility; lifestyle factors like smoking, excessive alcohol, obesity, and stress can diminish sperm quality. Early evaluation—ideally after six months of trying for women over 35 or sooner if risk factors exist—allows timely treatment options, improving the chances of a successful pregnancy.
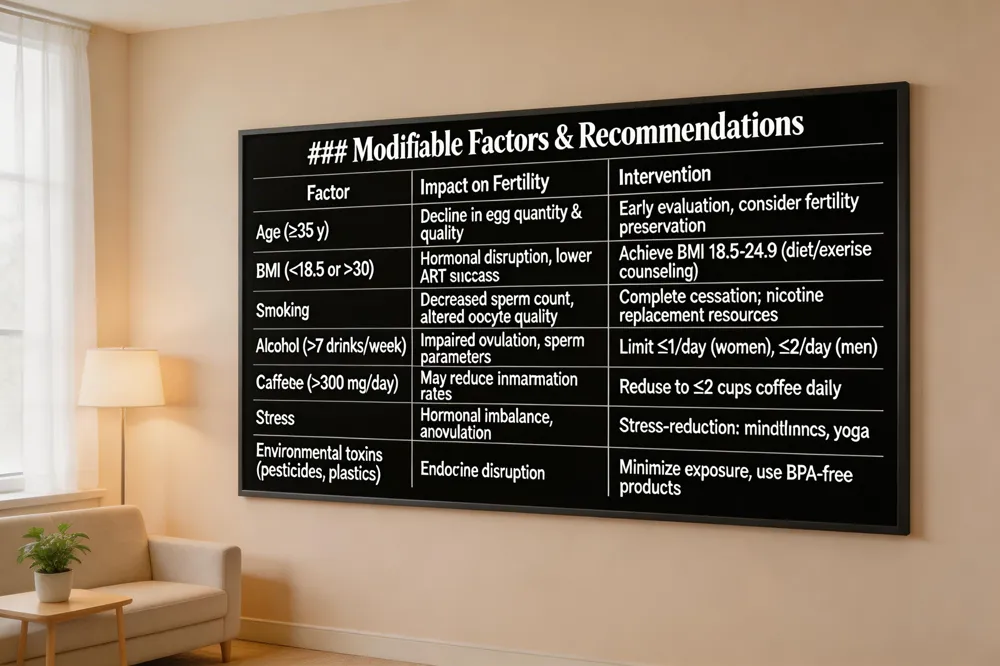 Female fertility begins to decline noticeably after the mid‑30s, with a sharp drop in egg quantity and quality after age 35 and a further decline after age 40. This age‑related decline makes early evaluation especially important for women who are 35 or older, as timely diagnosis and treatment can improve pregnancy chances.
Body‑mass index (BMI) outside the normal range (BMI < 18.5 or > 30) disrupts hormonal balance and ovulation; obesity (BMI > 30) is linked to reduced ovulation and lower success rates of assisted reproductive technologies, while underweight can also suppress ovarian function. Smoking, heavy alcohol use, and chronic stress are modifiable risk factors that lower fertility in both partners and may lead to menstrual irregularities, anovulation, and poorer treatment outcomes.
Pre‑conception counseling should address these lifestyle factors, encouraging weight‑loss or weight‑gain to achieve a healthy BMI, smoking cessation, limiting alcohol to moderate levels, and stress‑reduction techniques such as mindfulness or regular exercise. Community resources in Queens, NY—such as the RMA Queens Fertility Center, local health department workshops, and low‑cost reproductive health screenings—provide accessible education and support for women preparing to conceive.
Early warning signs that merit a fertility work‑up include menstrual irregularities (cycles < 21 days, > 35 days, or absent periods), painful periods, heavy or prolonged bleeding, chronic pelvic pain or dyspareunia, and recurrent miscarriage. Other clues are hirsutism, acne, unexplained weight changes, or a history of sexually transmitted infections, pelvic inflammatory disease, endometriosis, or prior abdominal surgery. Women over 35 should seek evaluation after six months of unprotected intercourse; those under 35 after a full year, but any of the above red‑flags justify earlier consultation. Prompt assessment—through detailed history, hormone panels, transvaginal ultrasound, and hysterosalpingography—can identify ovulatory disorders, tubal blockage, uterine abnormalities, or diminished ovarian reserve while treatment options remain most effective.
Raveco, a woman‑led OB‑GYN practice in Queens, NY, offers same‑day transvaginal ultrasounds, hysterosalpingograms, and comprehensive hormone testing on site. With easy subway access (7, E, F, M lines) and a average four‑to‑six‑week wait for specialist appointments, Raveco provides personalized, culturally competent care to help Queens residents move quickly from symptom recognition to a tailored fertility plan.
.png)
Compassionate care for every stage of womanhood. Visit one of our convenient locations or book your appointment online today.

