
Navigating Menopause: A Complete Guide to Hormone Therapy
Hormone Replacement Therapy Explained for Menopausal Women
Navigating Menopause: A Complete Guide to Hormone Therapy
Follow us here:



Uterine fibroids affect 70–80 % of pre‑menopausal women in the United States, often causing heavy bleeding, pelvic pain, and infertility concerns. Diagnosis begins with a pelvic exam followed by imaging—transabdominal or transvaginal ultrasound is the first line, while MRI or hysterosonography clarifies size, number, and location for treatment planning. Shared decision‑making should integrate symptom severity, desire for future fertility, and personal health goals. Discuss the full spectrum of options: hormonal therapies (e.g., GnRH agonists, LNG‑IUD) for short‑term control; uterus‑preserving procedures such as myomectomy, uterine artery embolization, or MRI‑guided focused ultrasound; and definitive hysterectomy when childbearing is complete. Consider recovery time, potential risks, cost, and the impact on quality of life to choose the approach that aligns with each woman’s values. Open dialogue with a gynecologist ensures the plan reflects both medical evidence and personal preferences.
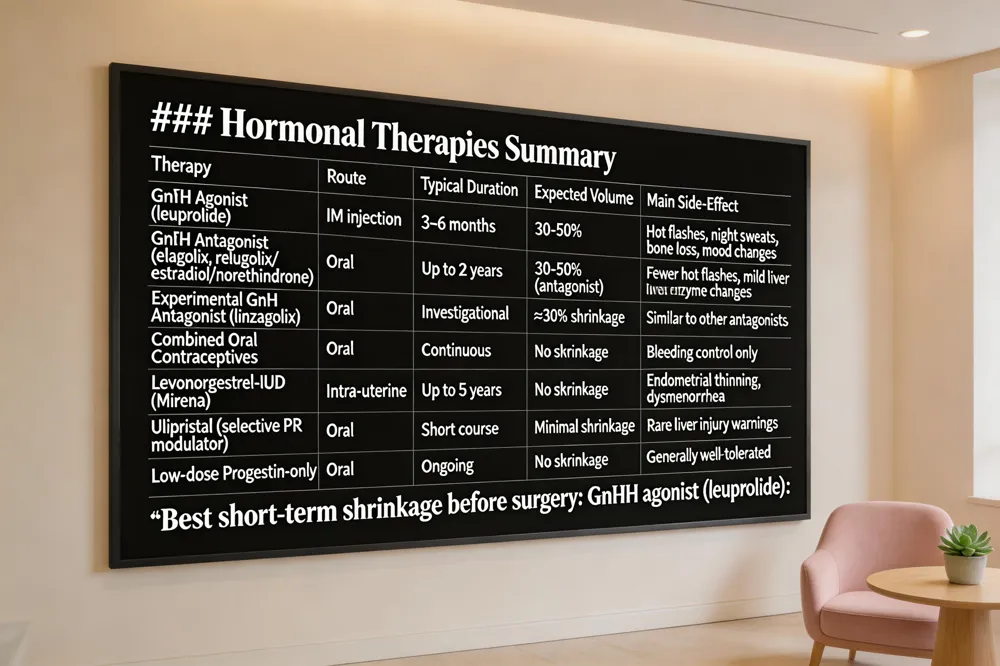 Uterine fibroids respond to several hormone‑based medicines that aim to shrink the tumors or control bleeding. GnRH agonists and antagonists such as leuprolide (Lupron) or elagolix create a temporary menopause‑like state, lowering estrogen and progesterone. Agonists are usually given by injection for 3‑6 months and can reduce fibroid volume by 30‑50 %, while antagonists can be taken orally for up to two years with fewer hot‑flash symptoms. Oral tablet options include GnRH antagonists (relugolix/estradiol/norethindrone) and, experimental agents like linzagolix (Yselty) that have demonstrated measurable shrinkage. Conventional birth‑control pills lessen bleeding but do not shrink fibroids, and ulipristal carries rare liver‑injury warnings. Levonorgestrel‑releasing IUDs (Mirena) thin the endometrium, dramatically decreasing menstrual loss, yet they do not reduce fibroid size and may be unsuitable when the uterine cavity is distorted. Hormone‑replacement considerations: after hysterectomy or during menopause, low‑dose progestin‑only regimens or GnRH‑based add‑back therapy can protect bone density while keeping estrogen low enough to avoid stimulating fibroid growth. Nutritional support: a Mediterranean‑style diet rich in leafy greens, berries, green tea, probiotic yogurt, eggs, omega‑3 fish, and nuts supplies antioxidants and anti‑inflammatory compounds that may aid hormone balance and modestly shrink fibroids. Tablets to shrink fibroids – Yes, oral GnRH antagonists (e.g., elagolix) and experimental linzagolix can reduce size; traditional pills cannot. Best hormonal treatment – Short‑term GnRH agonists (leuprolide) provide the greatest shrinkage before surgery. Side‑effects – Hot flashes, night sweats, bone loss, mood changes, spotting, weight gain, and rare clot risks; monitoring is essential. Can you take HRT with fibroids? – Yes, but low‑dose estrogen‑limiting regimens (progestin‑only or GnRH‑based) are preferred to avoid stimulating growth. 7 foods for shrinking fibroids – Spinach, kale, berries, green tea, yogurt, eggs, salmon, and nuts, eaten regularly, support hormone metabolism and may lessen fibroid size.
 Uterine fibroids affect 70‑80 % of pre‑menopausal women in the United States, and the choice of surgery hinges on fertility goals, symptom severity, and long‑term health risks.
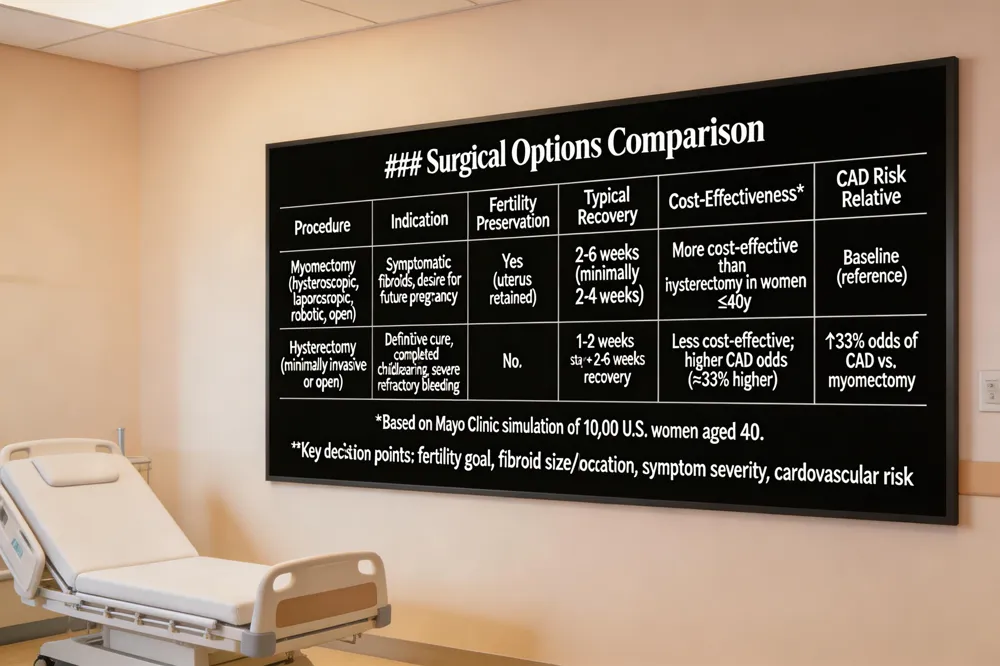
Myomectomy techniques and fertility preservation – Myomectomy removes only the fibroids while sparing the uterus, making it the gold‑standard for women who wish to conceive. It can be performed hysteroscopically for submucosal lesions, laparoscopically or robot‑assisted for intramural or subserosal tumors, or via a traditional laparotomy for very large or numerous fibroids. Minimally invasive approaches reduce blood loss, limit scarring, and typically allow a return to normal activities within two to six weeks.
Hysterectomy as definitive cure – Hysterectomy eliminates the uterus and all fibroids, providing permanent symptom relief and eliminating recurrence. It is reserved for women who have completed childbearing, have severe refractory bleeding, or when malignancy is suspected.
Cost‑effectiveness and coronary artery disease (CAD) risk – A Mayo Clinic simulation of 10,000 U.S. women aged 40 showed myomectomy to be more cost‑effective than hysterectomy while delivering comparable quality‑of‑life benefits. Hysterectomy was associated with up to a 33 % higher odds of CAD compared with myomectomy, underscoring the importance of weighing cardiovascular risk in treatment planning.
Recovery timelines by surgical approach – Minimally invasive hysterectomy (laparoscopic, robotic, or vaginal) often requires an overnight stay and a two‑to‑four‑week recovery, whereas an open abdominal hysterectomy can extend convalescence to six weeks. Myomectomy recovery varies: hysteroscopic and laparoscopic cases heal in 2‑4 weeks, while open myomectomy may need 4‑6 weeks.
Key patient‑focused questions –
Choosing the optimal pathway involves shared decision‑making with a trusted OB/GYN, integrating personal goals, health status, and the latest evidence.
 Uterine fibroids are traditionally treated with surgery, but a growing portfolio of uterus‑preserving options now lets many women avoid incisions.
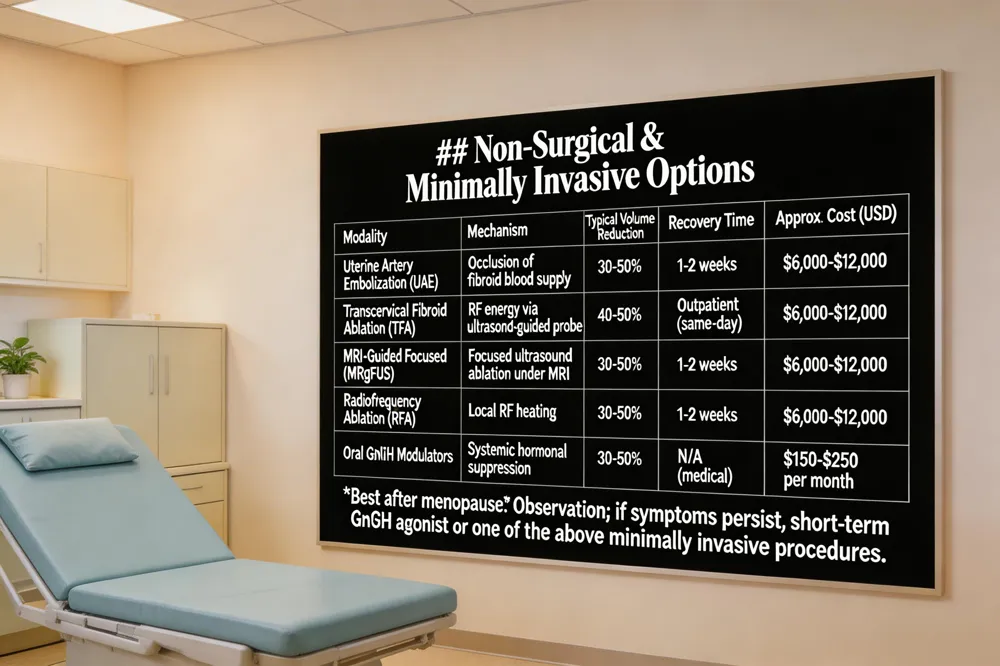
Uterine artery embolization (UAE) blocks fibroid blood flow with tiny particles delivered through a catheter, shrinking lesions by 30‑50 % and relieving heavy bleeding. Recovery is usually 1‑2 weeks, and most insurers cover the procedure when medically indicated.
Transcervical fibroid ablation (TFA) uses a thin, ultrasound‑guided probe inserted through the vagina to deliver radio‑frequency energy that contracts fibroid tissue by 40‑50 %. It is an outpatient, incision‑free option that rapidly eases bleeding and pelvic pain.
MRI‑guided focused ultrasound (MRgFUS) focuses high‑energy sound waves on fibroids under MRI guidance, thermally ablating tissue without any incision. Although effective, insurance coverage can be variable, making it less accessible for some patients.
Radiofrequency ablation (RFA) techniques—whether transcervical or laparoscopic—offer similar volume reduction with short recovery times and uterus preservation.
New treatment for fibroids without surgery: TFA and other RFA methods provide a cutting‑edge, non‑surgical alternative that eliminates stitches and hospital stays, delivering symptom relief within weeks.
Cost: UAE, RFA and MRgFUS typically range from $6,000‑$12,000 per treatment; oral hormone modulators (e.g., Oriahnn, Myfembree) average $150‑$250 per month.
Best after menopause: Most fibroids shrink naturally; observation is often sufficient. Persistent symptoms may be managed with short‑term GnRH agonists or minimally invasive procedures like TFA, UAE, or endometrial ablation.
Overall treatment pathway: Begin with watchful waiting, then consider hormonal therapy, followed by minimally invasive options (UAE, MRgFUS, RFA/TFA) before surgical myomectomy or hysterectomy, based on symptom severity, fibroid characteristics, and fertility goals.
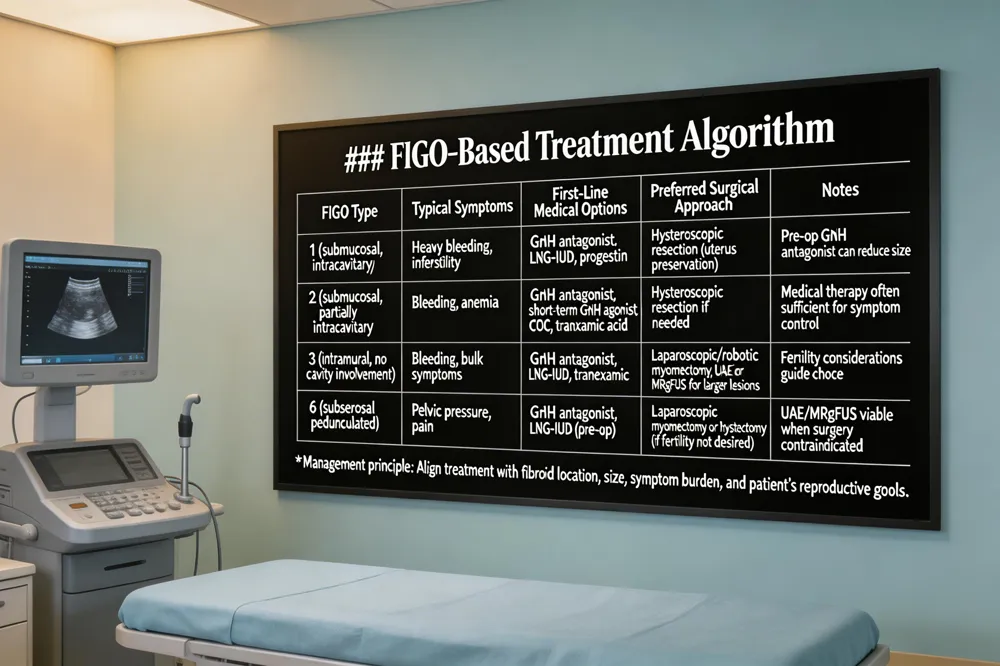 Uterine fibroids are classified by FIGO type, which directs a location‑specific treatment strategy while balancing fertility goals and symptom control.
FIGO 1 (submucosal, intracavitary) – These lesions often cause heavy bleeding and infertility. Initial management favors medical therapy—GnRH antagonists, oral progestins, or a levonorgestrel‑releasing IUD to reduce bleeding and shrink the fibroid. If uterine preservation is desired, hysteroscopic resection is the preferred surgical option, allowing precise removal with minimal uterine trauma. A combined pre‑operative GnRH antagonist followed by hysteroscopic or laparoscopic surgery enhances outcomes when the fibroid is large.
FIGO 2 (submucosal, partially intracavitary) – GnRH antagonists (e.g., relugolix) rapidly lower volume and improve anemia while preserving fertility. Short‑term GnRH agonists can be used pre‑operatively. Levonorgestrel‑IUDs, combined oral contraceptives, or tranexamic acid control bleeding. When medical therapy is insufficient, hysteroscopic resection remains the minimally invasive surgical choice.
FIGO 3 (intramural, no cavity involvement) – Initial therapy includes GnRH antagonists, LNG‑IUDs, or tranexamic acid for bleeding control. Persistent symptoms or fertility wishes may be addressed with minimally invasive myomectomy (laparoscopic, robotic, or hysteroscopic). Larger or multiple lesions can be managed with uterine artery embolization or MRI‑guided focused ultrasound. Hysterectomy is reserved for definitive cure after childbearing.
FIGO 6 (subserosal pedunculated) – Surgical removal, typically laparoscopic myomectomy or hysterectomy when fertility is not a concern, is the definitive option. Pre‑operative GnRH antagonists or LNG‑IUDs can reduce size and bleeding. Minimally invasive alternatives such as uterine artery embolization or MRI‑guided focused ultrasound are viable when surgery is contraindicated. Multidisciplinary, patient‑led counseling ensures the chosen pathway aligns with individual reproductive plans and health status.
.png)
Compassionate care for every stage of womanhood. Visit one of our convenient locations or book your appointment online today.

