
Your Guide to a Safe and Successful VBAC
Preparing for a VBAC Delivery Plan
Your Guide to a Safe and Successful VBAC
Follow us here:



Uterine fibroids affect up to 80 % of women by age 50, with prevalence reaching 70 % in Caucasian and over 80 % in African‑American populations. These benign tumors are a leading cause of heavy menstrual bleeding, anemia, pelvic pain, urinary urgency and infertility, profoundly diminishing daily comfort, work productivity and emotional well‑being. Over the past decade, patients and providers have moved away from hysterectomy toward uterus‑preserving, minimally invasive options that spare fertility and shorten recovery. Laser‑assisted fibroid treatment (LIFT) exemplifies this shift: using a fiber‑optic laser delivered hysteroscopically or laparoscopically via a precise pathway, it precisely coagulates fibroid tissue while preserving surrounding myometrium. Clinical data show 40‑70 % volume reduction, 80‑90 % symptom relief and rapid return to normal activities, making LIFT a compelling, patient‑centered alternative for women seeking symptom relief while maintaining reproductive potential and health.
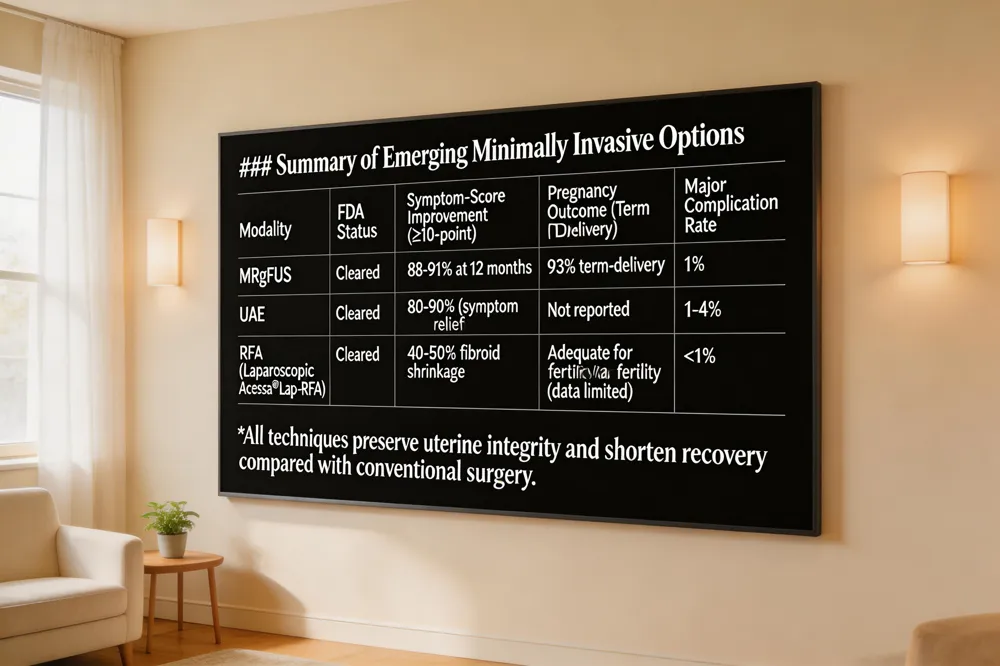 Non‑surgical modalities are reshaping uterine fibroid care. Magnetic resonance‑guided focused ultrasound (MRgFUS) is a fully non‑invasive, FDA‑cleared treatment that uses MRI‑guided high‑intensity sound waves to thermally ablate fibroids without incisions. Clinical trials show 88‑91% of patients achieve a ≥10‑point symptom‑score improvement at 12 months and pregnancy outcomes are favorable (93% term‑delivery rate). Uterine artery embolization (UAE) blocks fibroid blood flow with embolic particles, providing symptom relief in 80‑90% of cases and a major‑complication rate of only 1‑4 %. Radiofrequency ablation (RFA), including the laparoscopic Acessa® Lap‑RFA delivers controlled heat via a thin needle, shrinking fibroids by 40‑50% and enabling same‑day discharge. Patients report rapid return to work (≈3 days) and high satisfaction, though larger or numerous fibroids may require repeat treatment. Overall, these minimally invasive options offer effective symptom control, preserve uterine integrity, and shorten recovery compared with traditional surgery.
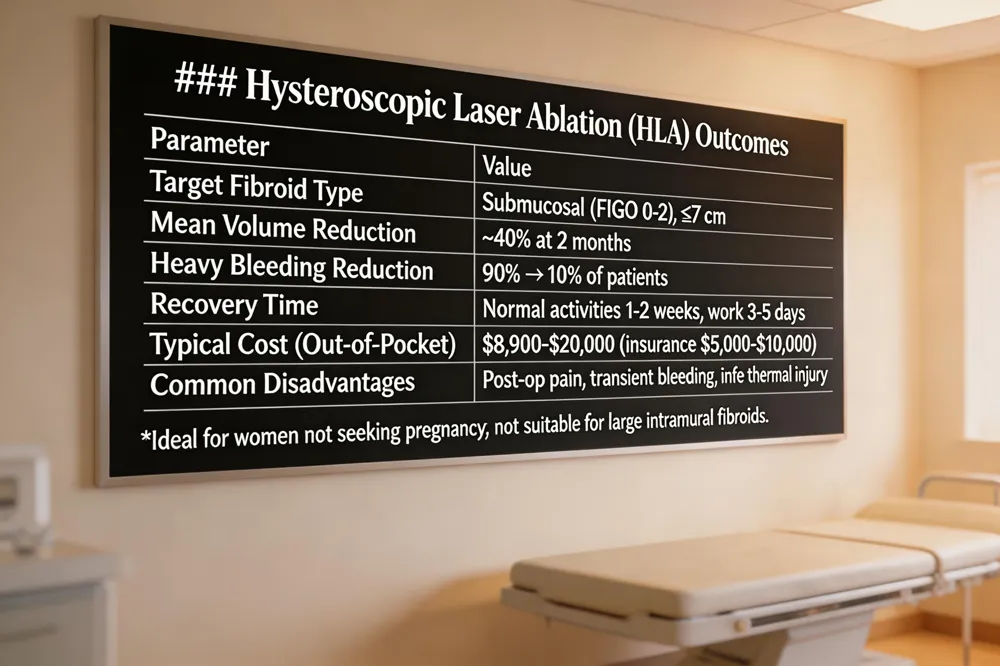 Laser treatment for fibroids – Hysteroscopic laser ablation (HLA) uses a 980‑1470 nm diode laser inserted through a hysteroscope to vaporize the core of submucosal fibroids (FIGO 0‑2, ≤7 cm). In a pilot study, mean volume fell ~40 % at 2 months and heavy bleeding dropped from 90 % to 10 % of patients. The uterus is preserved, no incisions are made, and recovery is rapid.
Hysteroscopic laser ablation – This office‑based procedure delivers focused energy that coagulates fibroid tissue while sparing surrounding myometrium. It is ideal for women with symptomatic submucosal lesions who are not seeking pregnancy; patients report only mild cramping and spotting for a few days.
Laser fibroid removal recovery time – Most women resume normal activities within 1–2 weeks, returning to work in 3–5 days. Light lifting should be avoided for about a week.
Disadvantages of laser ablation – Possible postoperative pain, transient bleeding, infection, and rare thermal injury to adjacent tissue. Larger or deep intramural fibroids are less suitable.
Can fibroids be treated with laser? – Yes; submucosal fibroids ≤7 cm respond well. Intramural or larger lesions often require other modalities such as MRgFUS, RFA, or laparoscopic myomectomy.
Laser fibroid removal cost – Out‑of‑pocket costs range $8,900–$20,000; insurance typically reduces this to $5,000–$10,000. Prices vary by facility and insurance coverage.
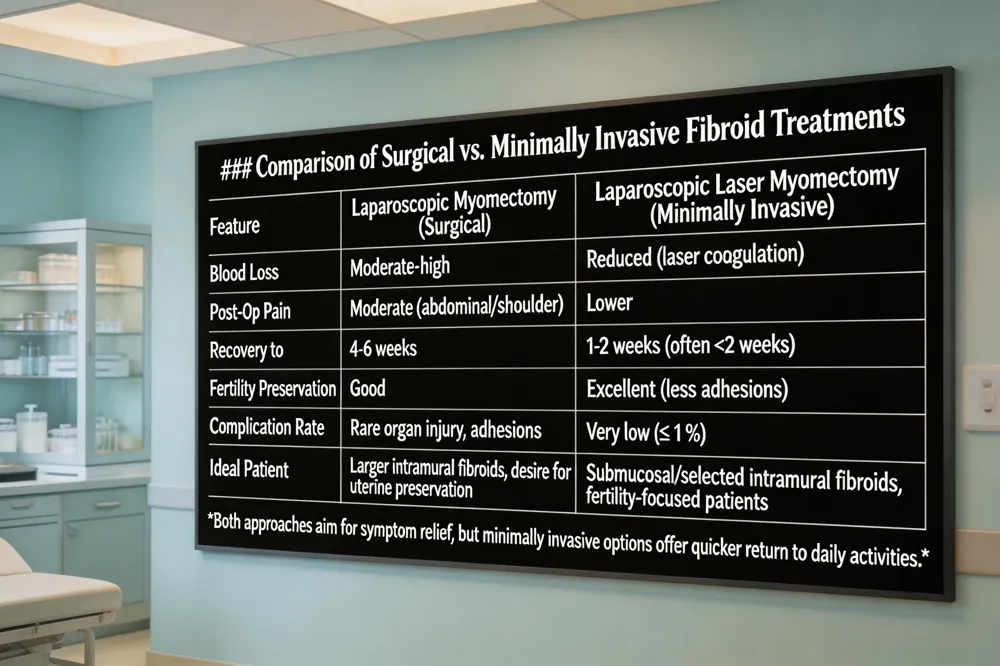 Laparoscopic myomectomy, the traditional uterus‑sparing surgery, is generally safe but can cause postoperative abdominal or pelvic pain, shoulder discomfort from insufflation, bruising at the small port sites, low‑grade fever, and occasional vaginal spotting or fluid collections. Rare complications include organ injury, adhesions that may affect future pregnancies, or deep infection.
Laparoscopic laser myomectomy uses a precision fiber to cut and coagulate fibroid tissue, markedly reducing intra‑operative blood loss and postoperative pain. The laser’s focused energy seals vessels, leading to quicker recovery and better fertility preservation—especially valuable for women in Queens, NY, seeking personalized, women‑led care.
Patient‑reported symptom relief after fibroid removal is high: most women experience lighter bleeding, less pelvic pressure, and improved quality of life within weeks, with full recovery typically by 4‑6 weeks.
Treatment is tailored to FIGO classification. Submucosal type 1 fibroids (≤3 cm) are most often managed hysteroscopically with laser ablation or morcellation, preserving the uterine cavity and fertility. Intramural type 3 fibroids are addressed with minimally invasive options such as uterine‑artery embolization, MR‑guided focused ultrasound, or laparoscopic myomectomy/robotic myomectomy, depending on symptom severity and reproductive goals.
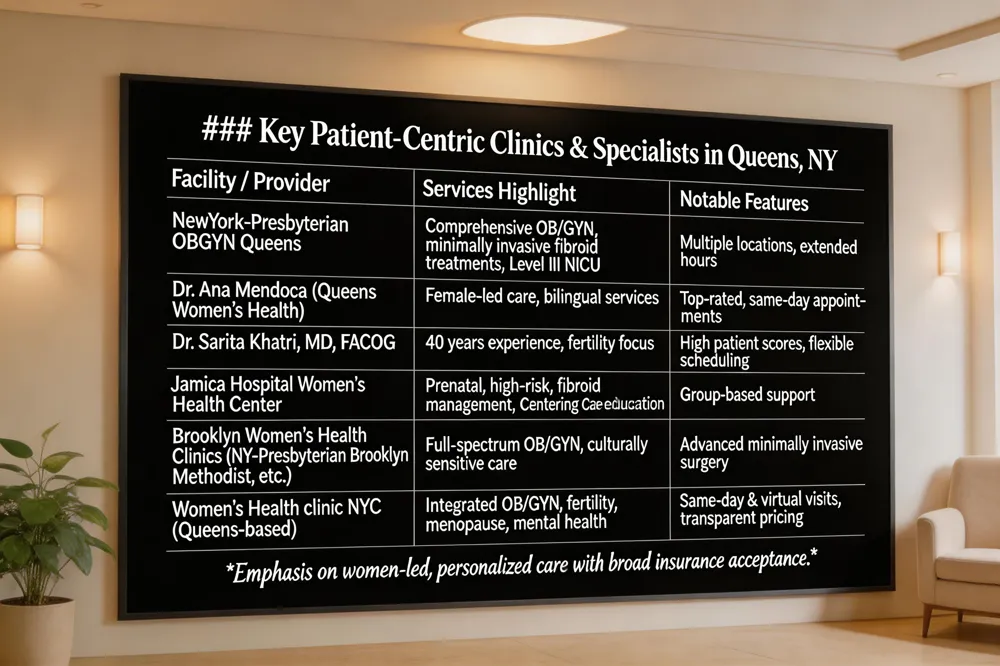
NewYork‑Presbyterian Queens offers a comprehensive OB/GYN practice with board‑certified physicians, routine exams, family‑planning, prenatal testing, fertility services, and minimally invasive fibroid treatments. Multiple locations, including Hollis, provide extended hours and a Level III NICU.
Top‑rated female specialists include Dr. Ana Mendoza (Queens Women’s Health), Dr. Liza Khan (Queens OB‑GYN Center), and Dr. Sarita Khatri, MD, FACOG), who brings 40 years of experience, bilingual care, and flexible same‑day or Saturday appointments.
The woman‑led team at Queens OB‑GYN Center, led by Dr. Sarita Khatri, consistently earns high patient scores. Riverside Women’s Health also provides advanced, individualized care and broad insurance acceptance.
Jamaica Hospital’s Women’s Health Center offers prenatal, high‑risk pregnancy, and fibroid management, with group‑based Centering Care education and a dedicated outpatient clinic.
NewYork‑Presbyterian Brooklyn Methodist, Trust Women’s Healthcare, and The Brooklyn Hospital Center’s Family and Women’s Health Center deliver full‑spectrum OB/GYN services, including minimally invasive surgery and culturally sensitive care.
A women‑led Queens clinic combines OB/GYN, fertility, menopause, and mental‑health services under one roof, offering same‑day and virtual visits, broad insurance coverage, and transparent pricing.
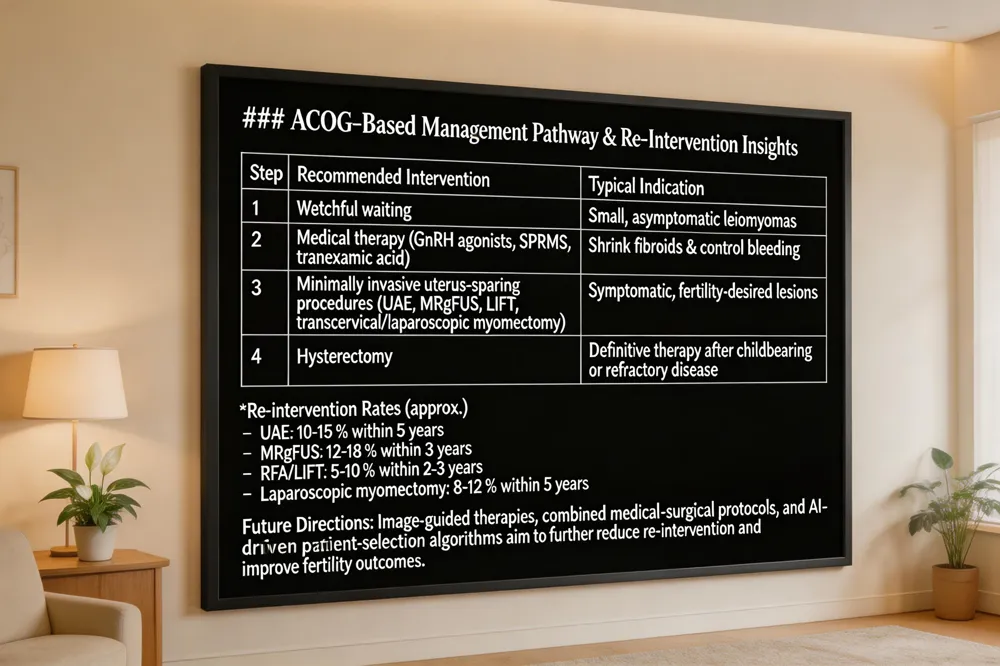 ACOG recommends a step‑wise, patient‑centered approach: watchful waiting for small, asymptomatic leiomyomas; medical therapy (GnRH agonists, SPRMs, tranexamic acid) to shrink fibroids and control bleeding; minimally invasive uterus‑sparing options such as transcervical or laparoscopic myomectomy, uterine artery embolization (UAE) link, MR‑guided focused ultrasound (MRgFUS) link, and laser‑assisted fibroid treatment (LIFT) link for larger or symptomatic lesions in women desiring fertility; and hysterectomy as definitive therapy after childbearing or for refractory disease.
FIGO type 2 (sub‑mucosal, partially intracavitary) lesions are best managed first with hysteroscopic resection; when surgery is unsuitable, medical pretreatment (GnRH analogues, LNG‑IUS, tranexamic acid) or combined hysteroscopic removal plus short‑term GnRH can be used.
FIGO type 6 (predominantly subserosal) fibroids generally require surgical removal—open or laparoscopic/robotic myomectomy—while observation or medical therapy is acceptable for asymptomatic cases.
Pre‑ and post‑treatment images illustrate the reduction or elimination of fibroids, aiding patient education. Surgical photos of myomectomy (open, laparoscopic, hysteroscopic) depict incision sites, intracorporeal removal, and uterine repair, providing realistic expectations for recovery.
Ongoing research is expanding the evidence base for laser‑assisted fibroid therapies and magnetic‑resonance‑guided focused ultrasound (MRgFUS). Large multicenter trials are evaluating newer laser wavelengths, real‑time thermal mapping, and volumetric MRgFUS protocols to improve non‑perfused volume ratios and reduce re‑intervention rates, especially in younger women. At the same time, patient‑centered initiatives are emphasizing shared decision‑making: clinicians provide clear, comparative data on symptom relief, recovery time, and fertility outcomes, while decision aids help women align treatment choices with personal goals. In Queens, women‑led practices are uniquely positioned to champion this model. By integrating culturally sensitive counseling, multidisciplinary expertise, and rapid outpatient access to laser and MRgFUS services, they empower patients to select uterus‑preserving, minimally invasive options that fit their lifestyles and reproductive plans.
.png)
Compassionate care for every stage of womanhood. Visit one of our convenient locations or book your appointment online today.

