
Decoding Your Prenatal Screening: What the Numbers Really Tell You
What Do Prenatal Screening Results Really Mean
Decoding Your Prenatal Screening: What the Numbers Really Tell You
Follow us here:



Sleep problems affect 40‑70 % of women during the menopausal transition, with hot flashes, night sweats, mood swings and anxiety often triggering frequent awakenings and non‑restorative sleep. Declining estrogen and progesterone disrupt temperature regulation and the brain’s GABA system, while stress and comorbid conditions such as sleep apnea can worsen insomnia. Because many of these factors are driven by hormonal fluctuations and lifestyle, non‑medication strategies are essential. They address the root causes—through consistent sleep‑wake schedules, cool dark bedrooms, screen‑free wind‑down routines, regular daytime exercise, and stress‑reduction techniques—without the risks of dependence, side effects, or contraindications associated with prescription sleep aids. Evidence‑based approaches like Cognitive Behavioral Therapy for Insomnia (CBT‑I) have shown durable improvements in sleep quality and overall well‑being, making them the preferred first‑line option for most menopausal women.
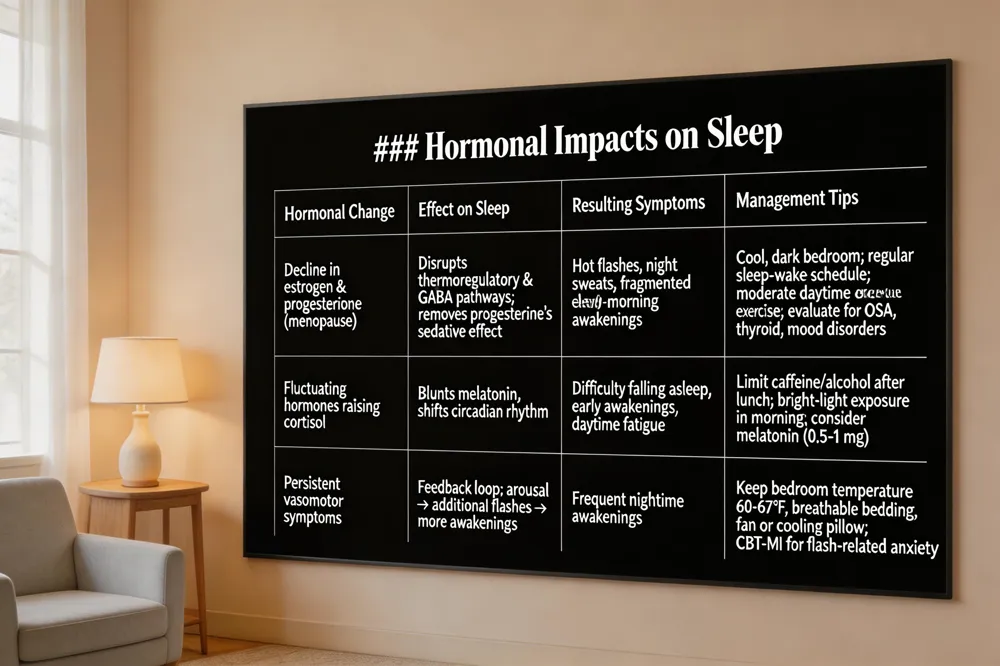 Estrogen and progesterone decline during the menopausal transition disrupt the brain’s thermoregulatory and GABA pathways, eliminating the natural sedative effect of progesterone and making it harder to stay asleep. The resulting vasomotor symptoms—hot flashes and night sweats—often awaken women and may even trigger additional flashes after a brief arousal, creating a feedback loop that fragments sleep. At the same time, fluctuating hormones raise cortisol and blunt melatonin, altering the circadian rhythm and contributing to early‑morning awakenings and daytime fatigue.
Menopause and sleeping too much – Because night‑time awakenings reduce restorative sleep, many women feel exhausted during the day and compensate with longer naps or oversleeping. The hormonal shift can amplify this cycle, but a regular sleep‑wake schedule, a cool, dark bedroom, and moderate daytime exercise help restore a healthier rhythm. Persistent daytime sleepiness warrants a medical check‑up to rule out sleep apnea, thyroid issues, or mood disorders.
Menopause insomnia how long does it last – Insomnia often begins in perimenopause and can persist for months or years after the final period, depending on the severity of hot flashes, mood changes, and stressors. Early lifestyle interventions—consistent bedtime, limiting caffeine/alcohol, and relaxation routines—shorten its duration. If sleep problems continue beyond three months and impair daily function, professional evaluation is recommended.
Does menopause insomnia go away – For many women, sleep improves as the body adapts to lower hormone levels, especially when hot flashes lessen. However, some experience lasting disturbances that require targeted treatment such as cognitive‑behavioral therapy for insomnia (CBT‑MI), hormone therapy, or treatment of co‑existing conditions like apnea. Individual timelines vary, so personalized care is essential.
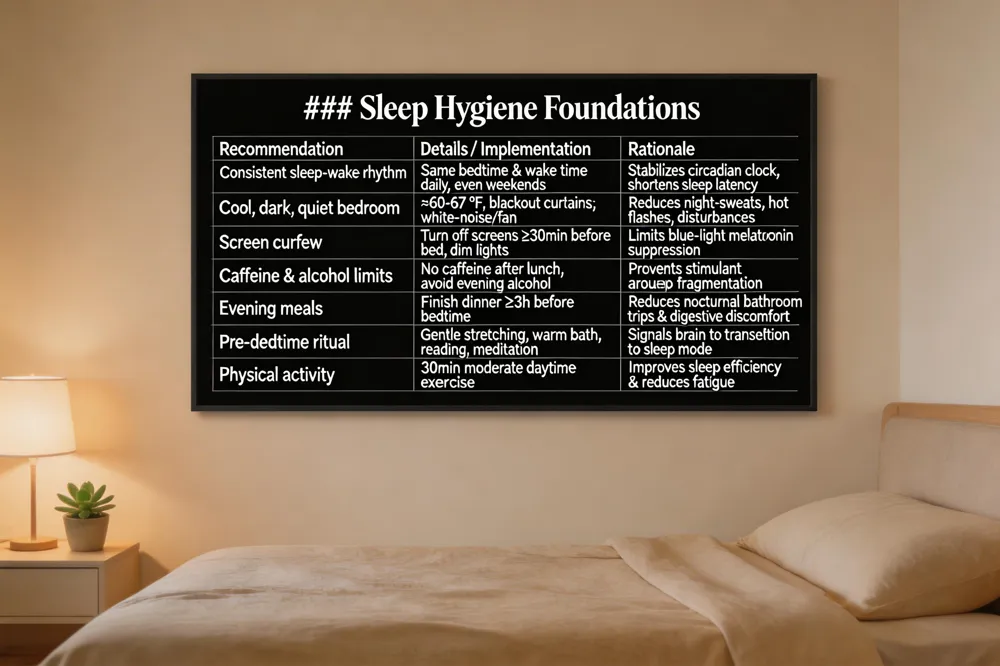 Set a sleep‑wake rhythm by going to bed and waking up at the same time each day, weekends, to stabilize the circadian clock and shorten latency. Keep the bedroom cool (≈60‑67 °F), dark and quiet; breathable bedding or a fan reduces night‑sweats and hot flashes. Turn off screens at least 30 minutes before bedtime and dim lights to limit blue‑light melatonin suppression. Limit caffeine after lunch, avoid evening alcohol, and finish meals three hours before sleep to prevent nocturnal bathroom trips.
What helps menopause sleep problems? – Cooling the sleep environment, a consistent schedule, limiting stimulants, a pre‑bedtime ritual (reading, gentle stretching, warm bath) and, if needed, CBT‑I or melatonin/prescription aids; hormone therapy may also lessen vasomotor symptoms.
Best over‑the‑counter aid – magnesium, which supports muscle relaxation and circadian regulation, is often most effective; melatonin, valerian or chamomile are alternatives but should be started low and discussed with a clinician.
Melatonin for menopause insomnia – supplemental melatonin can improve sleep onset and quality by realigning circadian rhythm, especially when insomnia is linked to delayed sleep‑phase; start with 0.5‑1 mg 30‑60 minutes before bed and consult a healthcare provider.
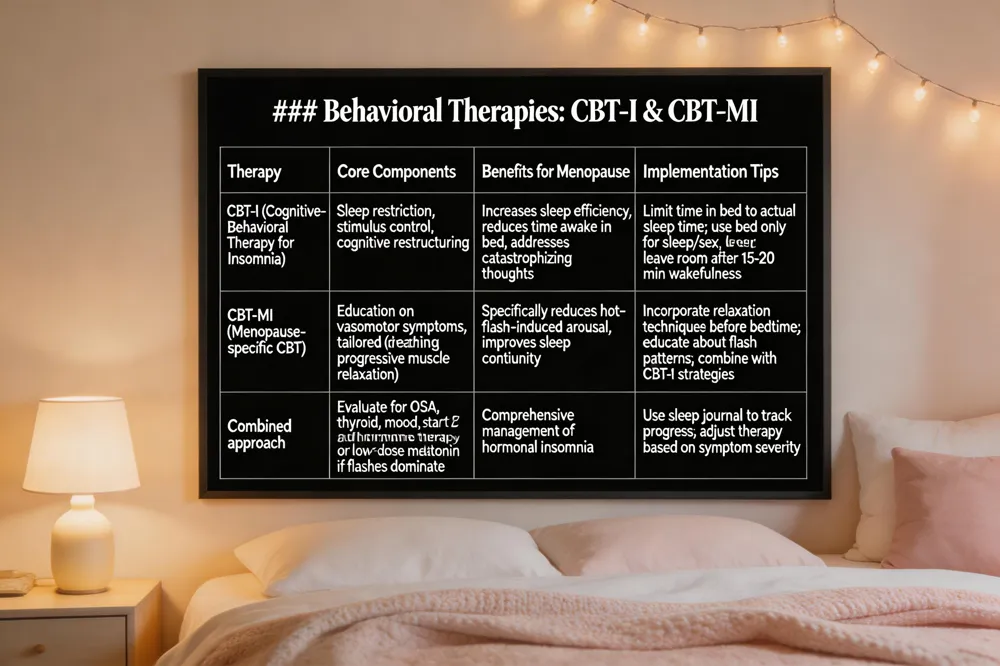 Cognitive‑Behavioral Therapy for Insomnia (CBT‑I) is the first‑line, non‑pharmacologic treatment for chronic insomnia in menopausal women. It combines sleep‑restriction (limiting time in bed to actual sleep duration) and stimulus‑control (using the bed only for sleep or sex, leaving the room after 15‑20 minutes of wakefulness) to rebuild sleep pressure and break the wake‑up‑in‑bed habit. Cognitive restructuring targets worries about night‑time awakenings, hot flashes, and hormone‑related mood swings, helping women replace catastrophizing thoughts with realistic expectations.
Menopause‑specific CBT (CBT‑MI) adds education about vasomotor symptoms and tailored relaxation techniques (deep breathing, progressive muscle relaxation) to reduce hot‑flash‑induced arousal. Both approaches improve sleep efficiency without medication side effects.
Postmenopausal insomnia treatment begins with a thorough evaluation to rule out sleep apnea or other disorders, then CBT‑I is offered; hormone therapy or low‑dose melatonin may be added when hot flashes dominate. Hormonal insomnia is first addressed by identifying the endocrine trigger, reinforcing sleep‑hygiene, and, if needed, using CBT‑I or brief hormone‑balancing therapy. To beat menopause insomnia, adopt a regular sleep‑wake schedule, a cool dark bedroom, limit caffeine/alcohol, use a calming bedtime routine, and consider CBT‑MI or CBT‑I for lasting relief.
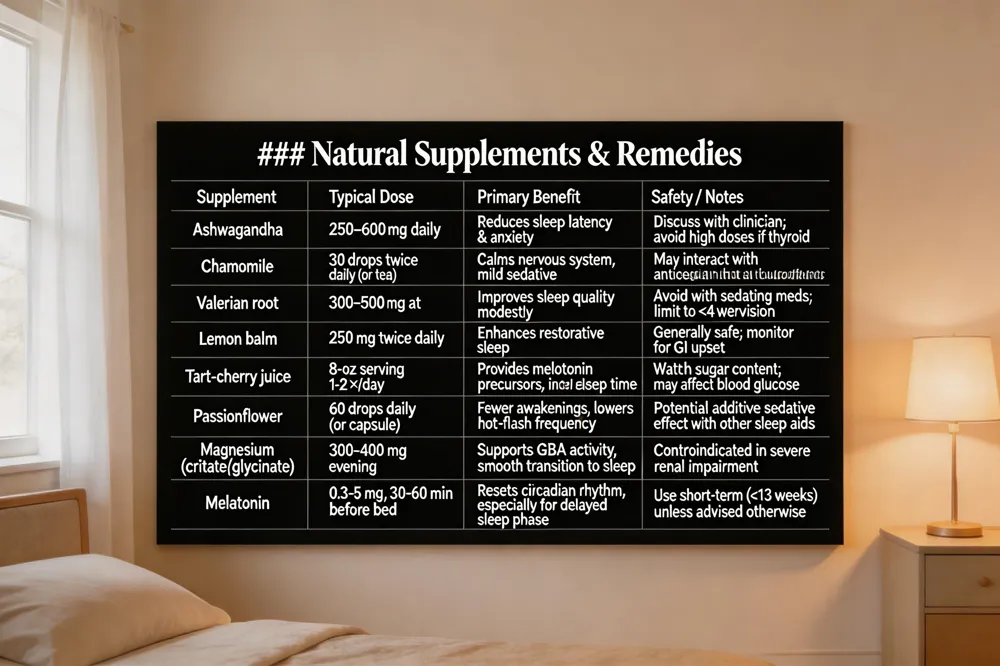 Menopause‑related sleep problems can often be eased with evidence‑based natural agents. Herbal options that have shown benefit include ashwagandha (250–600 mg daily) for reducing sleep latency and anxiety, chamomile (30 drops twice daily) to calm the nervous system, valerian root (300–500 mg at bedtime) for modest improvements in sleep quality, and lemon balm (250 mg twice daily) which may enhance restorative sleep. Tart‑cherry juice supplies melatonin precursors and can increase total sleep time, while passionflower extract (60 drops daily) has been linked to fewer nighttime awakenings and lower hot‑flash frequency.
Magnesium (300–400 mg of citrate or glycinate in the evening) supports GABA activity and can smooth the transition to sleep; melatonin (0.3–5 mg taken 30–60 minutes before bed) helps reset the circadian rhythm, especially when bedtime is irregular.
Safety considerations: Supplements are not universally regulated; dosages should be individualized, and potential interactions with prescription medications (e.g., SSRIs, HRT) must be reviewed. Women with kidney disease, heart conditions, or who are pregnant should avoid certain herbs.
Clinician consultation is essential before starting any regimen. A women's‑health provider can confirm the appropriateness of each supplement, monitor for side effects, and integrate them with lifestyle changes—consistent sleep‑wake times, a cool dark bedroom, limited caffeine/alcohol, regular daytime exercise, and relaxation techniques—to achieve the best sleep outcomes during menopause.
 During the menopausal transition, several health issues can compound sleep disruption. \ Obstructive sleep apnea (OSA) becomes two‑ to times times after moreod vessel because), estrogen the);one loss lesses the muscles that keep the airway open. Women with OSA may report loud snoring, gasping, or daytime fatigue and should be evaluated with a sleep study. \ Restless legs syndrome (RLS) affects many post‑menopausal women; low iron stores can worsen symptoms, so checking ferritin and supplementing iron when needed can reduce nighttime leg urges. \ Urinary urgency and increased nighttime bathroom trips are common, often linked to hormonal changes and pelvic floor laxity; limiting fluid intake a few hours before bed and practicing bladder‑training can lessen interruptions. \ Mood disorders such as depression and anxiety frequently accompany menopause and amplify insomnia. Addressing these with counseling, mindfulness, or appropriate medication improves both mood and sleep quality. \ What is severe insomnia during menopause? Severe insomnia is a persistent inability to fall asleep, stay asleep, or obtain restorative sleep that markedly interferes with daily life. Hormonal fluctuations trigger hot flashes and night sweats that fragment sleep, while depression or anxiety further disrupt sleep architecture. Management includes regular sleep schedules, a cool dark bedroom, limiting caffeine/alcohol, and cognitive‑behavioral therapy for insomnia; short‑term melatonin or prescription aids may be used under medical guidance, and treating hot flashes helps reduce insomnia severity.
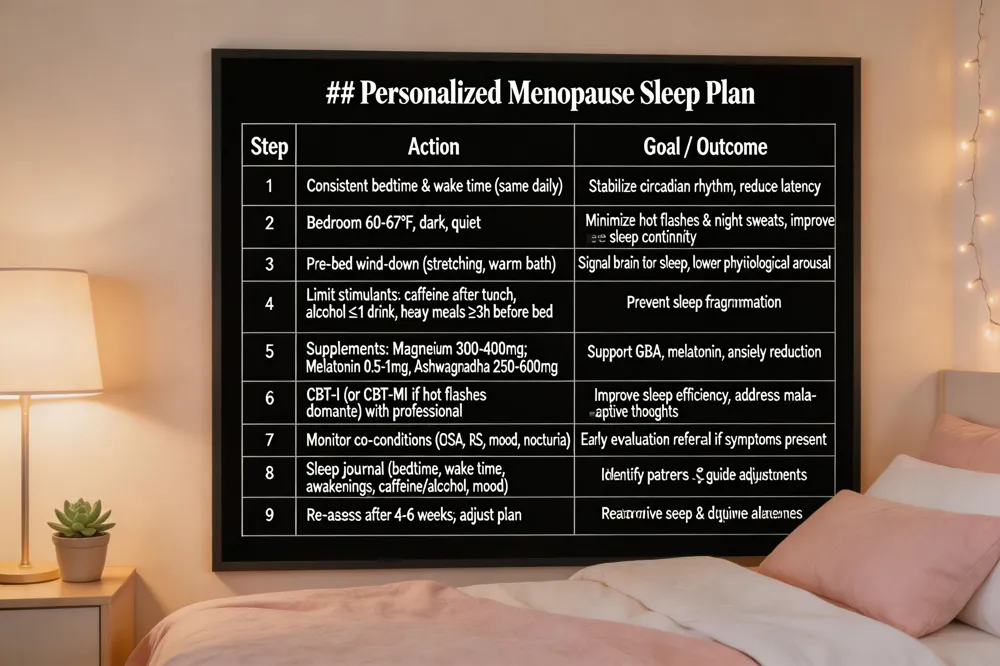 A successful menopause‑related sleep strategy blends evidence‑based sleep hygiene, targeted supplements, and cognitive‑behavioral therapy for insomnia (CBT‑I). Start by establishing a consistent bedtime‑wake schedule, keeping the bedroom cool (60‑67°F), dark and quiet, and limiting screen exposure, caffeine, alcohol, and heavy meals in the evening. Add a calming wind‑down ritual—such as gentle stretching, a warm bath, or soothing music—to signal the brain that it is time for rest. When night‑time hot flashes persist, short‑term melatonin (under 13 weeks) or magnesium can help stabilize the circadian rhythm, while ashwagandha or lemon‑balm may reduce anxiety; discuss any supplement with a clinician. CBT‑I, delivered by a trained women’s‑health professional addresses maladaptive thoughts, stimulus control, and sleep restriction, and has been shown to improve sleep continuity in menopausal women. Seek professional evaluation if insomnia lasts more than a few weeks, if you experience severe mood swings, loud snoring, or frequent nighttime bathroom trips, as these may signal sleep apnea or other medical conditions. Finally, track bedtime, wake time, awakenings, caffeine/alcohol intake, and mood in a sleep journal; patterns that emerge guide personalized adjustments and help your health‑care team fine‑tune the plan.
Medication‑free strategies can dramatically improve sleep during menopause. Keep a regular sleep‑wake schedule, avoid late‑day naps, and create a calming bedtime routine such as reading, gentle stretching, or a warm bath. Make the bedroom cool (60‑67 °F), dark and quiet, and limit screen exposure at least 30 minutes before sleep. Exercise earlier in the day, limit caffeine and alcohol after lunch, and choose light, easily digested evening meals. Mind‑body techniques—deep breathing, progressive muscle relaxation, or mindfulness meditation—reduce stress and hot‑flash intensity. For persistent problems, seek a women‑focused OB‑GYN who can assess hormonal, mood, and sleep‑disorder factors and guide personalized, evidence‑based care today.
.png)
Compassionate care for every stage of womanhood. Visit one of our convenient locations or book your appointment online today.

