
Your Quick Guide to Emergency Contraception
Emergency Contraception Facts You Should Know
Your Quick Guide to Emergency Contraception
Follow us here:



Sexual health, as defined by the World Health Organization, is a state of physical, emotional, mental, and social well‑being in relation to sexuality. It encompasses more than the absence of disease; it includes desire, arousal, comfort during intimacy, and the ability to communicate needs and boundaries. When any component—whether hormonal balance, stress levels, relationship dynamics, or societal attitudes—is disrupted, women may experience low libido, pain, or emotional distress that spill over into daily life. Maintaining optimal sexual health supports overall well‑being, improves mood, strengthens relationships, and can reduce the risk of conditions such as pelvic floor dysfunction, genitourinary syndrome of menopause, and even cardiovascular disease. Prompt attention to sexual concerns is therefore a vital part of comprehensive women’s health care.
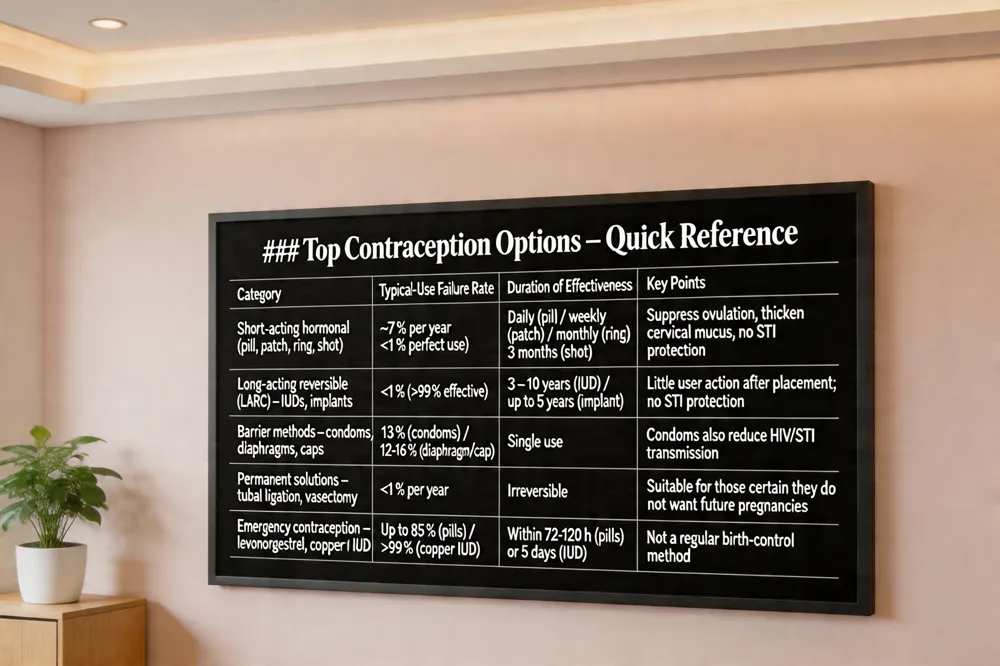 Short‑acting hormonal methods – These include combined oral contraceptive pills, progestin‑only pills, transdermal patches, vaginal rings, and the injectable progestin shot (Depo‑Provera). They work by suppressing ovulation and thickening cervical mucus. Typical‑use failure rates hover around 7 % per year, but perfect use lowers the risk to less than 1 %.
Long‑acting reversible contraceptives (LARCs) – Intrauterine devices (copper or hormonal) and subdermal implants (e.g., Nexplanon) are >99 % effective with typical use and require little or no user action after placement. They can protect for 3 – 10 years, making them the most reliable reversible options.
Barrier methods – Male and female condoms, diaphragms, and cervical caps physically block sperm. Condoms are the only contraceptives that also reduce the transmission of HIV and other STIs when used correctly (typical‑use failure ≈13 %).
Permanent solutions – Tubal ligation for women and vasectomy for men provide irreversible contraception with failure rates <1 % per year. These procedures are appropriate for those who are certain they do not want future pregnancies.
Emergency contraception – Levonorgestrel or ulipristal pills, taken within 72‑120 hours after unprotected intercourse, can prevent up to 85 % of pregnancies. Insertion of a copper IUD within five days offers >99 % effectiveness and ongoing protection.
What are the top 5 contraception methods?
Choosing the right method involves a personalized discussion with a qualified healthcare provider, taking into account medical history, lifestyle, and reproductive intentions.
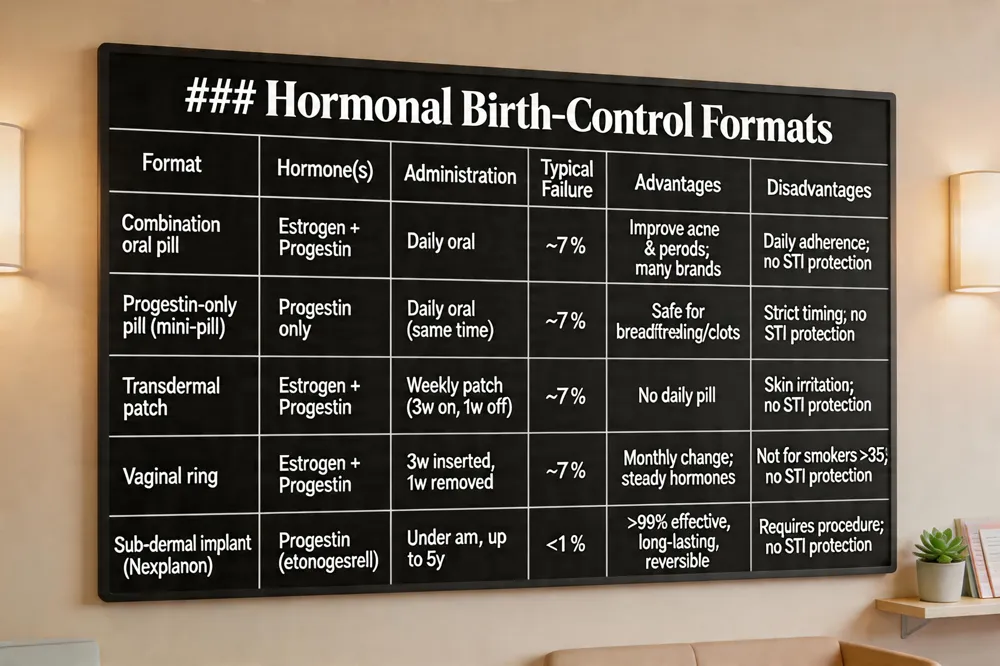 Hormonal contraception comes in several formats, each offering a balance of effectiveness, convenience, and side‑effect profile.
Combination vs. progestin‑only oral pills – Combination pills contain estrogen and progestin; they suppress ovulation and can improve acne, menstrual regularity, and dysmenorrhea. They are available as monophasic (same hormone dose each day) or multiphasic (varying doses) and in conventional 21‑day packs or extended‑use schedules. Low‑dose formulations reduce the risk of nausea and breast tenderness but may increase spotting. Progestin‑only pills (the “mini‑pill”) contain a single hormone, making them safe for breastfeeding women or those with estrogen‑related contraindications such as clotting disorders. However, they must be taken at the same time each day; a delay of more than three hours requires backup contraception.
Transdermal patch mechanics – The patch delivers estrogen and progestin through the skin, providing a steady hormone level that prevents ovulation and thickens cervical mucus. It is applied once a week for three weeks, followed by a patch‑free week for the withdrawal bleed. The patch eliminates daily pill‑taking, but like oral pills it does not protect against STIs, so condom use remains advisable.
Vaginal ring usage – A flexible silicone ring placed inside the vagina releases estrogen and progestin continuously for three weeks, then is removed for a week‑long hormone‑free interval. This once‑monthly method is over 99 % effective with typical use and offers the convenience of not having to remember daily dosing. Women who smoke, are over 35, or have a history of blood clots should avoid the ring.
Sub‑dermal implant details – The implant (e.g., Nexplanon) is a match‑stick‑sized rod inserted under the skin of the upper inner arm. It continuously releases the progestin etonogestrel, suppressing ovulation, thickening cervical mucus, and thinning the uterine lining, providing >99 % protection for up to five years. Insertion and removal are quick office procedures performed under local anesthesia. The implant is reversible, with rapid return to fertility after removal, but it does not protect against STIs, so condoms are recommended. Common side effects include altered menstrual bleeding patterns.
Choosing the right method depends on personal health history, lifestyle, and reproductive goals; a discussion with a qualified OB‑GYN or women’s‑health provider can help match you with the most suitable option.
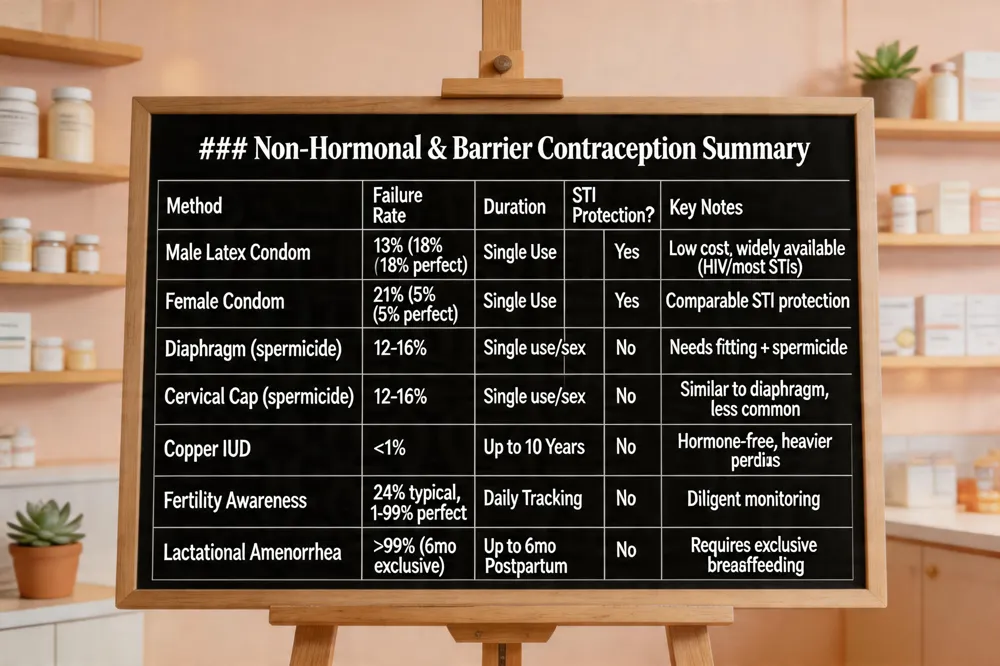 Barrier methods of contraception work by physically blocking sperm from reaching the egg. Male condoms and female condoms are the most widely used; male latex condoms reduce pregnancy risk to about 18 % with typical use (≈2 % with perfect use) and also provide reliable protection against most STIs, including HIV. Female condoms are slightly less effective (21 % typical, 5 % perfect) but offer a comparable STI shield. Diaphragms and cervical caps must be fitted by a clinician and are most effective when used with spermicide, yielding typical‑use pregnancy rates of roughly 12–16 %. Because they contain no hormones, these methods have no systemic side effects and are ideal for women seeking non‑hormonal, user‑controlled options.
Natural methods of contraception, often called natural family planning, rely on tracking fertility signals such as cycle length, basal body temperature, and cervical mucus. When practiced perfectly, fertility‑awareness can be 91‑99 % effective, but typical use drops to about 76 %. The lactational amenorrhea method can be >99 % effective for up to six months of exclusive breastfeeding. These approaches require daily observation and do not protect against STIs, so condoms remain essential for infection prevention.
For women who want the highest efficacy with minimal side‑effects, the copper intrauterine device is a hormone‑free option that is >99 % effective for up to 10 years, though it may cause heavier periods. Condoms also have negligible systemic effects and add STI protection, making them a low‑risk, highly versatile choice.
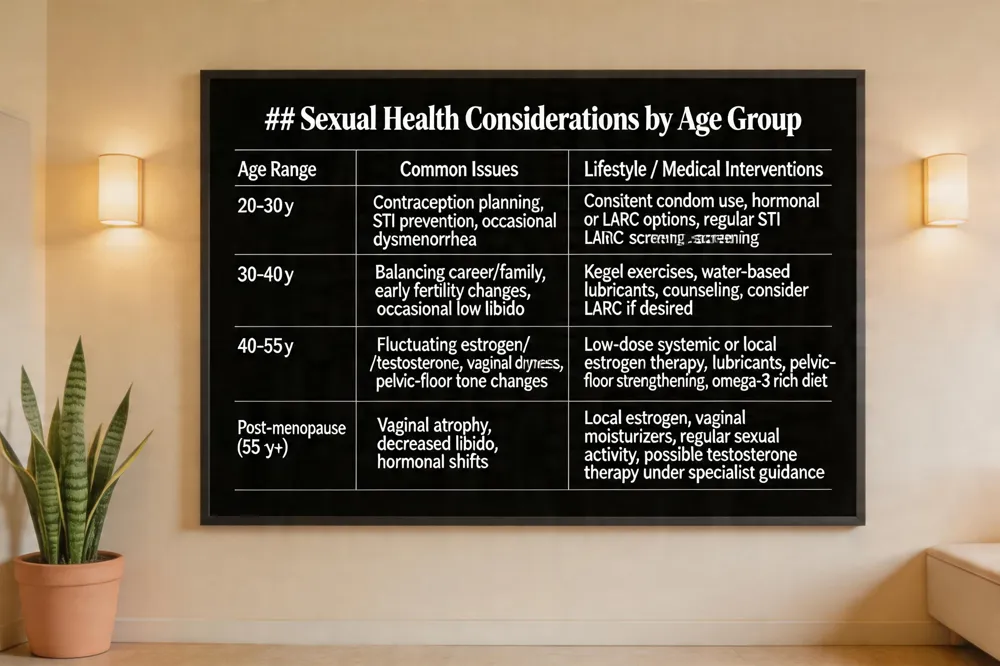 Sexual life after 40 years After age 40, fluctuating estrogen and testosterone can lower libido, cause vaginal dryness, and alter pelvic‑floor tone, making intercourse uncomfortable. Regular Kegel exercises, use of water‑based lubricants or vaginal moisturizers, and a diet rich in omega‑3 fatty acids and zinc support both comfort and desire. Open communication with a partner and stress‑reduction practices such as yoga, meditation, or counseling help counteract mental‑health impacts common in mid‑life. When symptoms persist, low‑dose systemic hormone therapy or localized estrogen may be prescribed by a qualified OB‑GYN to restore moisture and elasticity safely.
Women’s sexual health after menopause Menopause brings a marked estrogen decline, leading to vaginal atrophy, dryness, and decreased libido. Many women remain sexually active, but a sizable proportion experience desire, arousal, orgasm, or pain difficulties. Management includes consistent use of water‑based lubricants, vaginal moisturizers, and low‑dose local estrogen therapy when appropriate. Pelvic‑floor strengthening exercises improve tissue health and blood flow. Addressing mood changes, chronic illness, medication side effects, and relationship dynamics through counseling or therapy further enhances satisfaction. A personalized, comprehensive approach—combining medical treatment, lifestyle changes, and open communication—helps maintain a fulfilling sex life after menopause.
Women’s sexual health vitamins Key nutrients for sexual wellness are vitamin D (hormone regulation), B‑complex (energy and nerve function), magnesium (blood flow), and zinc (hormone balance). Botanical and amino‑acid supplements such as L‑arginine, chasteberry, maca, DHEA, ginseng, and red clover show modest benefits for libido or menopausal symptoms. A balanced diet usually supplies these nutrients; targeted supplementation is useful when deficiencies are identified. Always discuss new supplements with a healthcare professional, especially if you take prescription meds.
Women’s sexual health products Our curated line offers pH‑balanced, water‑based lubricants (LubeLife, Aloe Cadabra) suitable for daily use and toy‑friendly. Silicone options (Uberlube) provide a long‑lasting glide for extended sessions. Vaginal moisturizers (Daily V Soothe) address menopause‑related dryness, while pelvic‑floor trainers and kits support pelvic health and confidence. All items are sourced from women‑focused brands, ensuring quality and a medically informed approach to sexual wellness.
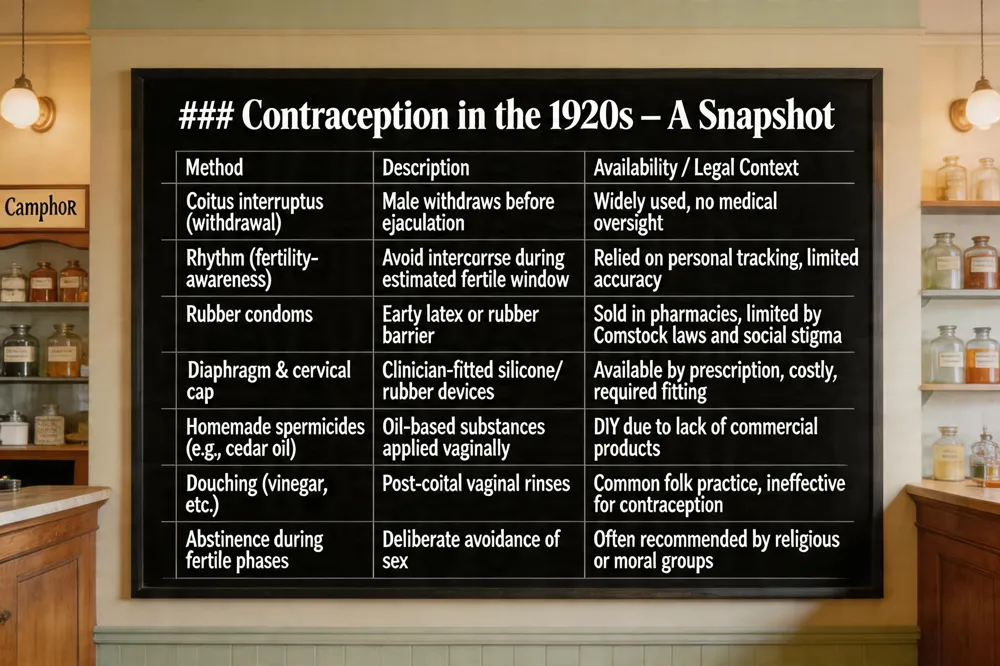 In the 1920s, couples relied on low‑tech methods such as coitus interruptus (withdrawal), the Rhythm Method (basic fertility awareness), and limited barrier devices like rubber condoms, diaphragms, and early cervical caps—often hard to obtain because of restrictive laws. Some women used homemade spermicides (e.g., cedar oil) or douching with vinegar after intercourse.
Early sexual‑health education was minimal; lessons on consent and body autonomy were rarely taught in schools, leaving many young people without reliable information about safe practices.
Stigma and communication barriers further impeded open discussions about sexuality. Cultural taboos and fear of judgment discouraged women from seeking professional advice, leading to reliance on informal knowledge and inconsistent use of available methods.
How did people avoid pregnancy in the 1920s? In the 1920s most couples relied on simple, often informal methods such as coitus interruptus (withdrawal and the “Rhythm Method,” a basic form of fertility awareness that avoided intercourse during the estimated fertile window. Barrier devices that were available included rubber condoms, diaphragms, and early cervical caps—though they were sold only in pharmacies or catalogues and could be hard to obtain because of the Comstock anti‑obscenity law. Some women used homemade spermicides—oil‑based substances like cedar oil or lead ointments—while others practiced douching with vinegar or other solutions after intercourse. Because reliable, widely marketed contraceptives were scarce, many relied on abstinence during certain parts of the cycle or on the limited barrier options that were accessible. Overall, contraception in the 1920s was a patchwork of low‑tech, often imperfect methods rather than the modern hormonal or long‑acting devices we have today.
 Guidelines for family planning – The CDC’s U.S. Medical Eligibility Criteria (MEC) and ACOG recommend a person‑centered counseling visit that reviews reproductive goals, medical history, lifestyle, and timing (post‑partum, post‑abortion, breastfeeding). Providers match each woman with a method that is safe and effective for her health status, schedule needed screenings (BP, anemia), and arrange follow‑up to monitor satisfaction and side‑effects.
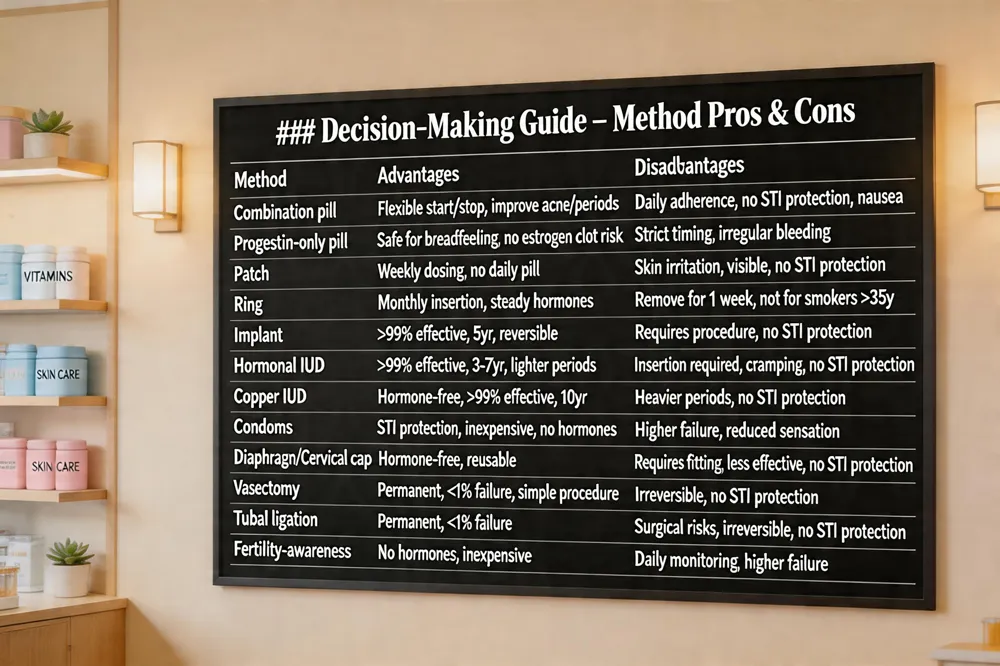
Types of family‑planning methods and their advantages and disadvantages – Hormonal options (pill, patch, ring, implant, hormonal IUD) offer >99% efficacy when used correctly but may cause mood changes, irregular bleeding, and no STI protection. Barrier methods (male/female condoms, diaphragms, cervical caps) are hormone‑free and protect against STIs, yet effectiveness hinges on perfect use and may reduce sensation. Long‑acting reversible contraceptives (LARCs) such as copper or hormonal IUDs and subdermal implants are >99% effective with minimal user action, but require insertion and do not guard against STIs. Permanent methods (tubal ligation, vasectomy) are irreversible and nearly 100% effective, suitable only for those certain no future pregnancy. Fertility‑awareness techniques are inexpensive and hormone‑free but demand daily tracking and have higher failure rates when not meticulously followed.
Best birth‑control pills with the side effects – Low‑dose combination pills (e.g., Lo Loestrin Fe, Sprintec®, Junel Fe) minimize nausea, breast tenderness, weight gain, and clot risk. Progestin‑only “mini‑pills” like Opill avoid estrogen entirely, reducing hormonal side‑effects and are safe for breastfeeding or smokers over 35. Choice should be individualized after reviewing personal health and prior experiences.
Can birth control cause high SHBG? – Yes. Combined estrogen‑progestin pills raise sex‑hormone‑binding globulin (SHBG), lowering free testosterone, which can affect libido, muscle mass, and bone health; the effect may linger for weeks after discontinuation.
 Finding a women's sexual health doctor means seeking a board‑certified OB‑GYN or sexual‑medicine specialist who evaluates low libido, pain during sex, hormonal shifts, and relationship stress. Look for a provider who offers trauma‑informed, multidisciplinary care—combining physical exams, hormone testing, pelvic‑floor therapy, counseling, and advanced options such as PRP or O‑Shot. Early education on consent, routine gynecologic visits (starting ages 13‑15) and regular STI screening (HIV at least once, chlamydia/gonorrhea annually under age 25 are part of comprehensive care.
For supplements that may support sexual wellness, modest evidence exists for L‑arginine/L‑citrulline (improves genital blood flow), maca root and damiana (traditional libido enhancers), aswagandha and chasteberry (stress‑related desire, menopause), and omega‑3 fatty acids (hormone synthesis and cardiovascular health). Discuss any supplement with your clinician to avoid interactions with prescription medications such as antidepressants or hormonal contraceptives.
Emergency contraception options include levonorgestrel (Plan B) taken within 72 hours, ulipristal acetate (ella) up to 120 hours, and a copper IUD inserted within five days of unprotected intercourse. Levonorgestrel cuts pregnancy risk by about 75 % when used promptly; ulipristal remains roughly 85 % effective through five days. The copper IUD not only serves as emergency contraception but also provides ongoing, highly effective birth control (failure < 1 %). These methods are for occasional use and may cause temporary nausea or spotting.
Begin by booking an appointment with a women‑led OB/GYN practice. During the visit the clinician will review your medical history, perform a pelvic exam, and ask about menstrual patterns, sexual desire, and any pain or discharge. Bring a list of current medications and past birth‑control experiences so the provider can tailor contraception counseling—whether you prefer a long‑acting reversible device, hormonal pill, barrier method, or other option. Together you can address STI screening, HPV vaccination, and symptoms of genitourinary syndrome of menopause. Outside the office, support your sexual well‑being with exercise, a diet rich in omega‑3s, adequate sleep, stress‑reduction techniques, and open communication with your partner about boundaries, desires, and concerns. These steps empower you to maintain optimal sexual health throughout life.
.png)
Compassionate care for every stage of womanhood. Visit one of our convenient locations or book your appointment online today.

