
Empowering Journeys: A New Standard for Maternal and Obstetric Excellence
Stories of Success in Obstetric Care
Empowering Journeys: A New Standard for Maternal and Obstetric Excellence
Follow us here:



The first fertility workup is both an emotional anchor and a medical compass for couples hoping to conceive. Early evaluation validates a couple’s concerns, reduces the anxiety of uncertainty, and opens a supportive dialogue about lifestyle changes, stress management, and realistic expectations. A structured workup—starting with a thorough history, targeted physical exam, timed hormone panels, transvaginal ultrasound, hysterosalpingogram, and semen analysis—pinpoints ovulatory disorders, tubal blockage, ovarian reserve issues, or male factor contributions, allowing clinicians to tailor treatment from ovulation induction to IVF or surgical correction. In Queens, a woman‑led clinic that emphasizes personalized care can further enhance outcomes by fostering trust, offering culturally sensitive counseling, and coordinating insurance and financial planning. This patient‑centered model ensures that every step, from diagnostic testing to therapeutic decision‑making, aligns with the couple’s values and goals, turning a daunting journey into a collaborative, hopeful experience.
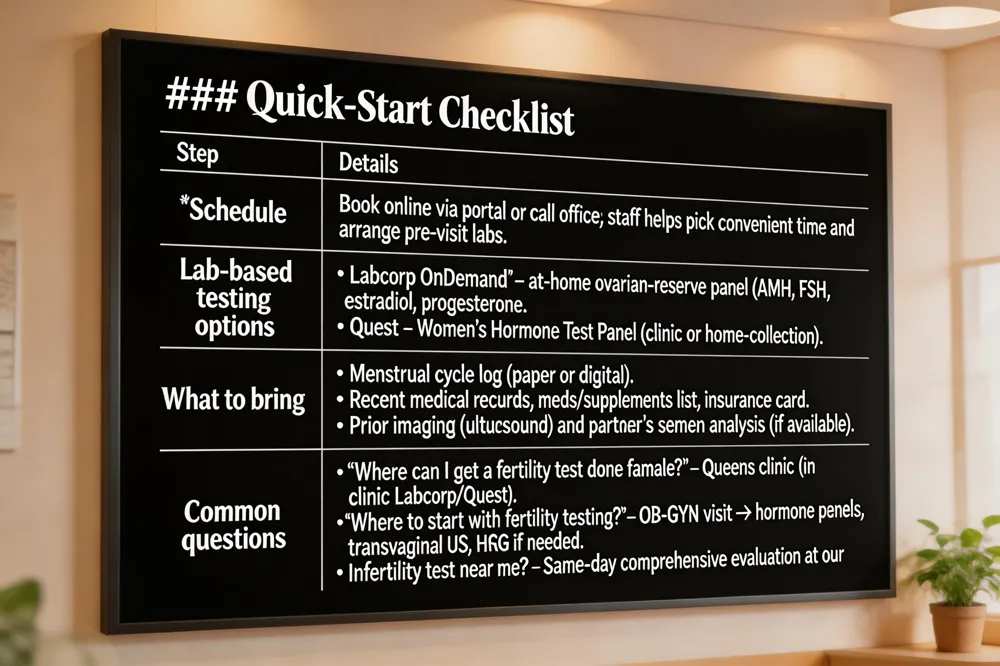 When you’re ready to begin a fertility work‑up, the first step is to schedule an appointment with our women‑led OB‑GYN practice in Queens, NY. You can book online through our website’s easy‑to‑use portal or call our office directly; our staff will help you pick a convenient time and coordinate any pre‑visit labs.
Lab‑based testing options – If you prefer to collect samples at home, Labcorp OnDemand offers at‑home kits for ovarian‑reserve panels (AMH, FSH, estradiol, progesterone). Quest also provides a Women’s Hormone Test Panel that can be done at a nearby Quest location or through a home‑collection kit. Both services deliver results securely online, but interpreting those numbers in the context of your personal history is essential. That’s why we ask you to bring the completed lab reports to your first visit, so our reproductive specialists can translate the data into a clear treatment roadmap.
What to bring – Prepare a notebook or digital calendar documenting your menstrual cycles, any fertility‑tracking methods you’ve used, and the dates of intercourse attempts. Gather recent medical records, a list of medications and supplements, and your insurance card. If you have previous imaging (ultrasound reports) or a partner’s semen analysis, bring those as well.
Answers to common questions
We look forward to supporting you on your family‑building journey with personalized, evidence‑based care.
 – A female fertility blood panel typically measures key hormones that reflect ovarian reserve and cycle health, including AMH, FSH, estradiol, LH, progesterone, TSH, and prolactin. Results, usually available within one to two weeks and guide discussions about natural conception, IVF, or egg‑freezing.
Fertility tests for females – Testing begins with hormone panels, followed by transvaginal ultrasound for antral follicle count and uterine anatomy, and an HSG to assess tubal patency. A day‑21 progesterone confirms ovulation, and a comprehensive ovarian reserve assessment aids IVF planning.
Infertility workup labs – The core lab work‑up includes early‑cycle FSH, LH, estradiol, AMH, prolactin, and TSH, plus a mid‑luteal progesterone. Male partner semen analysis and, when needed, testosterone testing run in parallel to pinpoint hormonal or reserve issues for a tailored treatment plan.
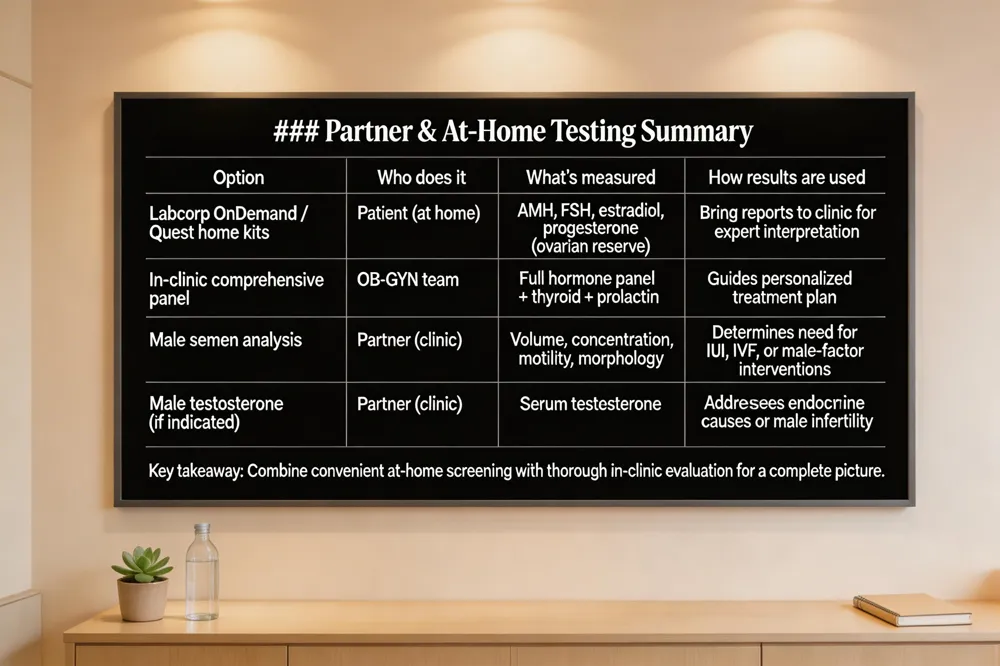 At‑home fertility test – At‑home kits can be a convenient first step, giving you a quick look at ovulation patterns, hormone levels or sperm health without leaving the house. However, they typically test only a few markers and may not capture the full picture of your reproductive health, especially if you have underlying conditions such as PCOS, thyroid disorders, or ovarian‑reserve concerns. Our Queens‑based, woman‑led practice offers comprehensive, clinically‑validated testing—including blood panels for AMH, FSH, estradiol, progesterone and thyroid function—performed in a comfortable, personalized setting. By combining the convenience of home screening with a thorough in‑clinic evaluation, we can pinpoint the exact cause of infertility and develop a tailored treatment plan. If you’ve tried a home test and want deeper insight, schedule an appointment with our obstetrics and gynecology team for a complete, expert assessment.
Where can I get a fertility test done female – You can have a comprehensive fertility evaluation performed at our Queens, NY women’s health clinic, where we offer personalized testing, counseling, and follow‑up care under the guidance of our female‑led OB‑GYN team. Labcorp OnDemand and Quest provide at‑home sample collection for ovarian‑reserve panels (AMH, estradiol, FSH) and other hormone assessments, with results delivered securely online. Bring those results to our clinic for expert interpretation and a treatment plan. Scheduling is easy via our website or by calling our office.
Infertility workup labs – A typical work‑up begins with early‑cycle serum hormone tests (days 2‑3): FSH, LH, estradiol, AMH, and prolactin to assess ovarian reserve, ovulatory function, and pituitary health. Thyroid‑stimulating hormone (TSH) screens for thyroid dysfunction, and a mid‑luteal progesterone level (around day 21) confirms ovulation. Parallel male evaluation includes a semen analysis—performed after 2‑5 days of abstinence—and, if indicated, serum testosterone. These coordinated tests guide a personalized treatment plan.
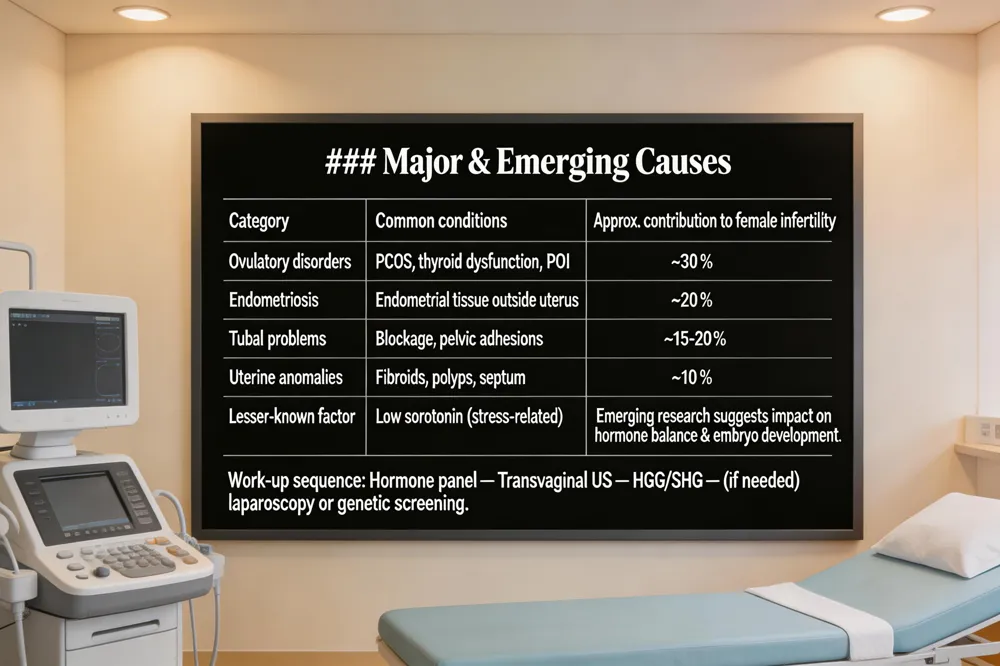 Infertility is defined as inability to conceive after 12 months of regular, unprotected intercourse (or after 6 months for women ≥ 35 years). The first step in a female work‑up is a detailed reproductive history, menstrual review, pelvic exam and baseline labs—Female blood hormone panel includes FSH, LH, AMH, estradiol, and progesterone. Ovulation is confirmed with a mid‑luteal progesterone level (≈day 21 of a 28‑day cycle). Imaging begins with a Transvaginal ultrasound assesses uterus, ovaries, and antral follicle count to assess ovarian reserve, uterine anatomy and antral follicle count; a Hysterosalpingogram (HSG) checks tubal patency with contrast dye follows when tubal patency or uterine abnormalities are suspected.
What are the top 3 causes of female infertility? The most common cause is an ovulatory disorder—conditions such as polycystic ovary syndrome (PCOS), thyroid dysfunction, or premature ovarian insufficiency (POI). Second is endometriosis, where tissue similar to the uterine lining grows outside the uterus and can impair egg release, fertilization or implantation. Third are tubal problems—blockage or pelvic adhesions that prevent sperm and egg from meeting. Together these three categories account for roughly half of female‑factor infertility cases.
Can low serotonin cause infertility? Emerging research suggests low serotonin may affect fertility. Serotonin is present in human oocytes, granulosa cells and early embryos; laboratory studies show it enhances estrogen and progesterone production, and serotonin‑deficient mice have smaller embryos and reduced gestation success. In humans, low‑serotonin states (often linked with depression) can increase stress and disrupt hormonal balance, indirectly lowering fecundability. While large clinical trials are pending, maintaining adequate serotonin is considered part of optimal pre‑conception health.
Infertility workup female Beyond the initial labs and ultrasound, further evaluation may include laparoscopy, genetic carrier screening, or referral to a reproductive endocrinologist for specialized treatment planning. Personalized care, lifestyle counseling, and timely intervention can dramatically improve a woman's chances of achieving pregnancy.
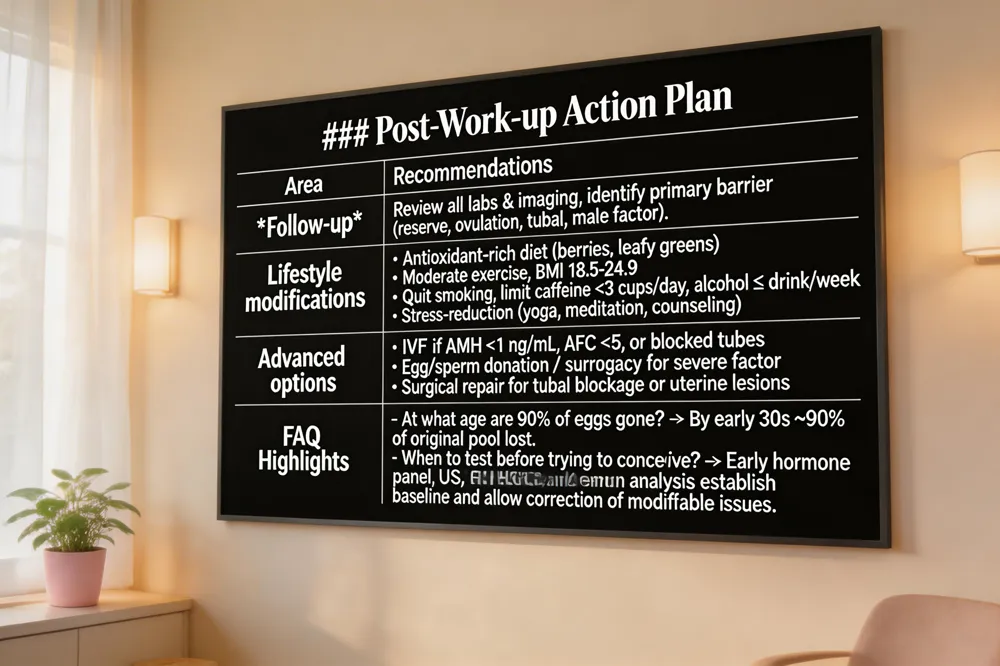 After the initial blood work, ultrasounds, HSG, and semen analysis are complete, the specialist reviews every result to pinpoint the primary barrier to conception and to design a personalized treatment plan. Elevated day‑3 FSH or low AMH signals diminished ovarian reserve, prompting earlier ovulation induction or consideration of assisted reproductive technologies. A normal‑aline‑phase progesterone >3 ng/mL confirms ovulation, while a blocked tube on HSG guides surgical repair or IVF. Male results showing low motility or abnormal morphology lead to repeat semen analysis, hormonal work‑up, or referral for varicocele surgery.
Lifestyle modifications that improve ovarian reserve and sperm health – Both partners benefit from a balanced antioxidant‑rich diet, regular moderate exercise, and a BMI in the 18.5–24.9 range. Quitting smoking, limiting caffeine to <3 cups/day, and reducing alcohol to ≤1 drink/week protect egg quality and sperm DNA integrity. Stress‑management techniques such as yoga, meditation, or counseling have been shown to normalize cortisol levels, which can improve ovulation regularity and sperm motility.
When to consider advanced options – If ovarian reserve is markedly low (AMH <1 ng/mL or AFC <5 follicles) or tubal blockage is confirmed, IVF becomes the most efficient route to pregnancy. Couples facing recurrent miscarriage, severe male factor infertility, or genetic concerns may discuss egg donation, sperm donation, or surrogacy as viable alternatives.
Frequently asked questions
You have taken the first courageous step toward building the family you envision, and we are here to guide you through a thorough, yet streamlined, fertility work‑up. First, we gather a detailed medical, menstrual, and lifestyle history from both partners, followed by a focused physical exam. Blood hormone panels (FSH, LH, AMH, estradiol, progesterone, TSH, prolactin) are timed to specific days of the menstrual cycle to assess ovarian reserve and ovulatory function. A transvaginal ultrasound provides antral follicle count, evaluates uterine anatomy, and detects cysts, polyps, or fibroids. Tubal patency is checked with a hysterosalpingogram or saline sonohysterogram, while the male partner contributes a semen analysis after 2–5 days of abstinence. If needed, additional testing such as genetic carrier screening or advanced sperm DNA fragmentation can be ordered. At our Queens clinic, each result is reviewed in a compassionate, personalized meeting, where we discuss how your unique profile informs treatment options—from lifestyle modifications and ovulation induction to IUI or IVF. We invite you to schedule your initial appointment today, bring your health records and a list of questions, and let us partner with you on this hopeful journey.
.png)
Compassionate care for every stage of womanhood. Visit one of our convenient locations or book your appointment online today.

