
Decoding Your Prenatal Screening: What the Numbers Really Tell You
What Do Prenatal Screening Results Really Mean
Decoding Your Prenatal Screening: What the Numbers Really Tell You
Follow us here:



Infertility is defined as the inability to achieve pregnancy after 12 months of regular, unprotected intercourse (or after six months when the woman is 35 years or older, or sooner if risk factors such as irregular cycles, tubal disease, or recurrent miscarriage are present). Starting the evaluation promptly—after one year of trying for women under 35, after six months for those over 35, and immediately for high‑risk situations—allows clinicians to identify hormonal imbalances, ovarian reserve issues, tubal blockages, or male factor problems before they become entrenched. Early detection offers several advantages: it clarifies the underlying cause, guides timely lifestyle modifications (weight management, smoking cessation, stress reduction), and enables the selection of the most effective treatment pathway, whether that is medication, surgery, or assisted reproductive technologies. By acting early, couples reduce the emotional strain of prolonged uncertainty and improve their overall chances of a successful, healthy pregnancy.
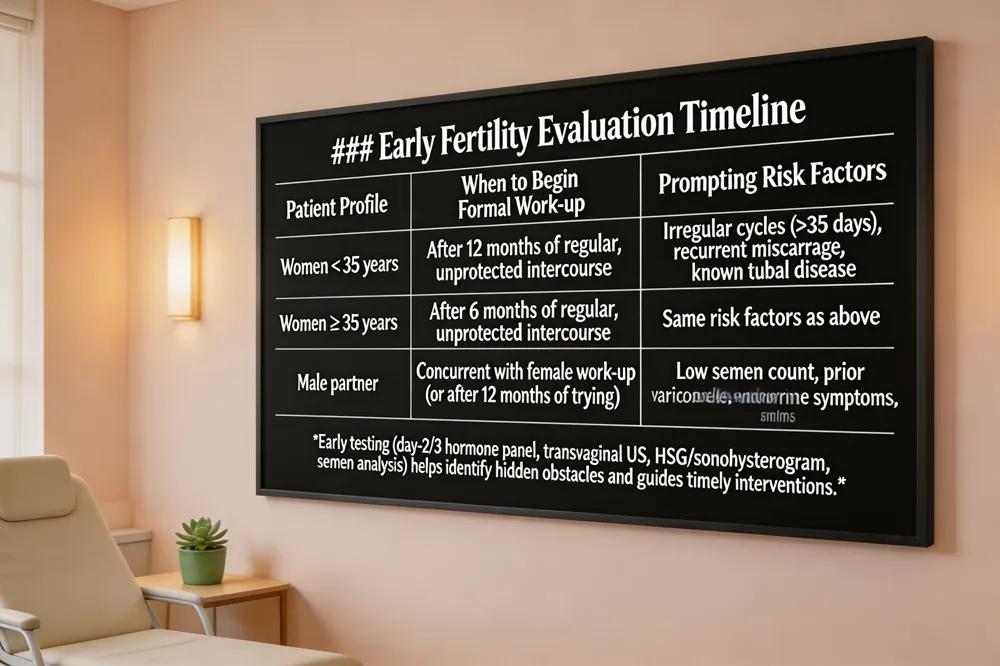 Most clinicians advise that couples begin a formal fertility work‑up after 12 months of regular, unprotected intercourse if the woman is under 35, or after 6 months if she is 35 or older. Irregular menstrual cycles (longer than 35 days), a history of recurrent miscarriage, or known tubal disease also prompt earlier evaluation. Early testing can uncover hidden obstacles before months exhausting months of trying. Typical first‑line studies include a day‑2–3 hormone panel (FSH, LH, estradiol, AMH, progesterone, prolactin, thyroid‑stimulating hormone) to gauge ovarian reserve and endocrine health, a transvaginal ultrasound for antral follicle count and uterine anatomy to count antral follicles and assess uterine anatomy, and a hysterosalpingogram or sonohysterogram to confirm fallopian‑tube patency. For the male partner, a semen analysis after 2‑5 days of abstinence evaluates count, motility, morphology, volume and pH. Age matters most; ovarian reserve declines steeply after the mid‑30s, and irregular cycles often signal ovulatory dysfunction. By testing early, you gain a clear roadmap—whether that means lifestyle changes, fertility preservation, or moving forward with confidence when you’re ready to try.
Infertility workup female
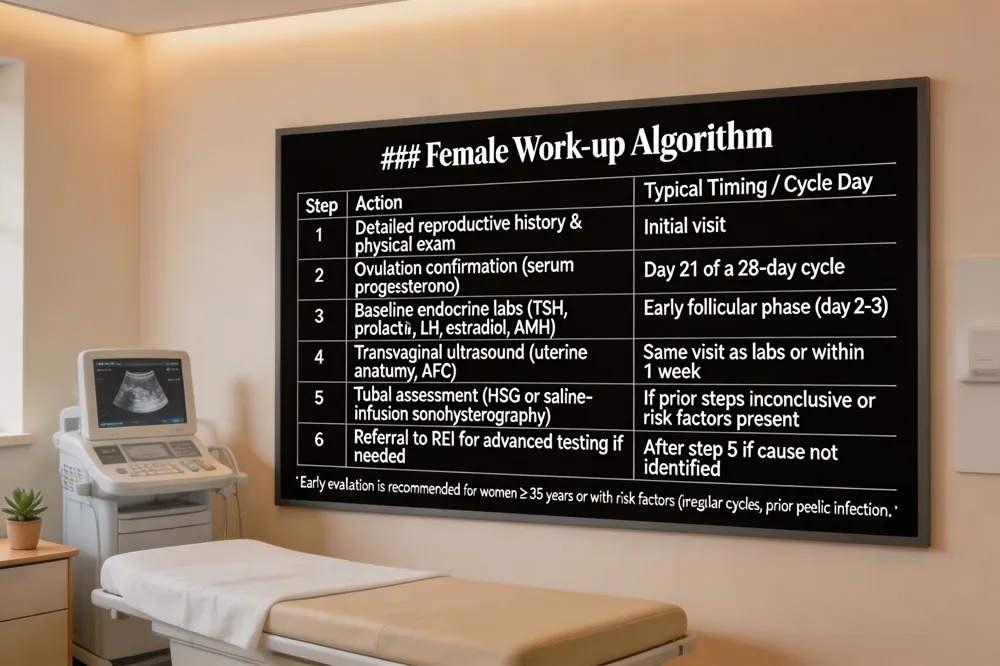
A female infertility work‑up begins with a thorough reproductive history and physical exam. Baseline hormone panels — including TSH, prolactin, early‑follicular‑phase FSH, LH, estradiol, and anti‑Müllerian hormone (AMH)—assess ovarian reserve and endocrine health. Ovulation is confirmed by a serum progesterone level around day 21 of a 28‑day cycle. A transvaginal ultrasound evaluates uterine anatomy and counts antral follicles. If initial studies are inconclusive, a hysterosalpingogram (HSG) or saline‑infusion sonohysterography checks tubal patency and uterine cavity. Women ≥ 35 years, or those with irregular cycles, endometriosis, or prior pelvic infection, should be evaluated after six months of trying rather than twelve. Lifestyle counseling—especially weight management for BMI > 30—is integral.
Female infertility workup algorithm
Infertility workup labs
Key female labs: AMH (egg quantity), day‑2/3 FSH & estradiol (ovarian response), LH (ovulation timing), progesterone (mid‑luteal), prolactin (hyperprolactinemia), and TSH (thyroid function). Male partner testing starts with a semen analysis; hormone panels (FSH, LH, testosterone, prolactin) may follow abnormal results.
Female infertility guidelines
Infertility is defined as 1 year of regular unprotected intercourse (6 months if ≥ 35 years). Evaluation follows a stepwise, cost‑effective approach: history, exam, ovulation confirmation, basic endocrine labs, and imaging. Early work‑up is recommended for irregular cycles, known uterine/tubal disease, endometriosis, or diminished ovarian reserve. Lifestyle modifications and shared decision‑making are emphasized.
Top 3 causes of female infertility
Fertility tests for females
After a year (or six months if ≥ 35) of trying, testing includes history, pelvic exam, hormone panel (FSH, LH, estradiol, progesterone, AMH), a transvaginal ultrasound, and, when needed, a HSG to assess tubal patency.
Blood test for fertility female
A day‑3 blood draw measures AMH (ovarian reserve), FSH, estradiol, and often progesterone. Results guide timing of conception, egg‑freezing decisions, or IVF planning.
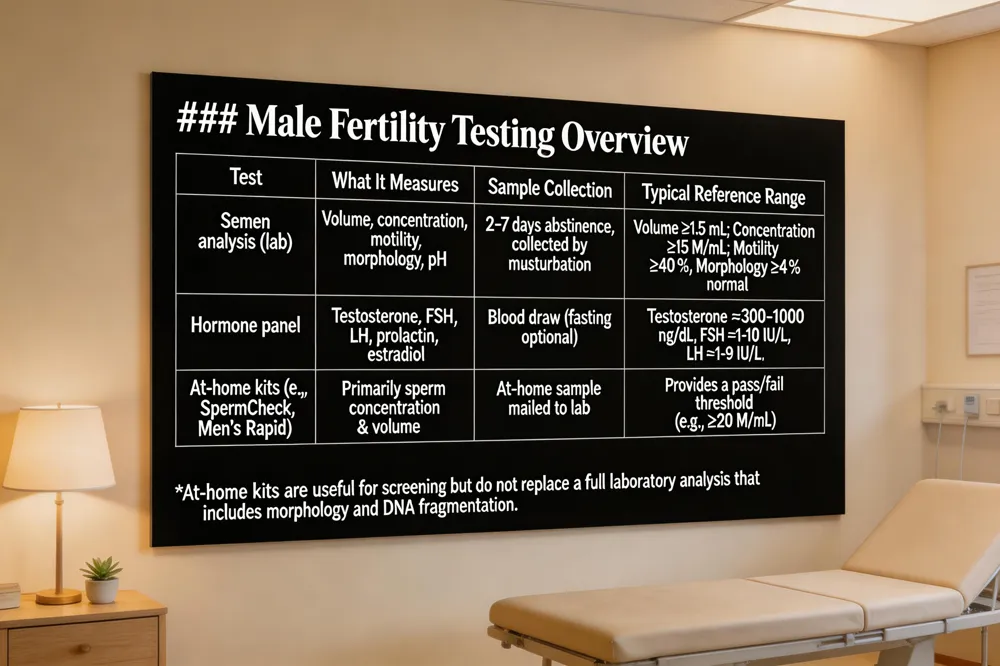 Semen analysis basics A semen analysis is the cornerstone of male fertility testing. After 2‑7 days of abstinence, the sample is collected (typically by masturbation in a private room) and evaluated for volume, sperm concentration, motility, morphology, pH. These parameters reveal the quantity and functional quality of sperm and help identify issues such as low count, poor movement, or abnormal shape.
Hormone testing for men When semen results are borderline or a history suggests endocrine involvement, blood work is added. Key hormones include testosterone, follicle‑stimulating hormone (FSH), luteinizing hormone (LH), prolactin, and estradiol. Abnormal levels can point to primary or secondary hypogonadism, pituitary disorders, or other metabolic problems that affect spermatogenesis.
At‑home male fertility kits For privacy and convenience, kits like SpermCheck, Men’s Rapid Fertility Test, or YO™ Male Fertility Test let you collect a sample at home. Results are typically available within 24‑48 hours and focus on sperm concentration and volume. While useful for screening, they do not replace a full laboratory analysis that includes morphology, DNA fragmentation, and hormone panels.
Where to get testing in Queens Queens residents can obtain a professional semen analysis at local fertility clinics, urology offices, or through partnered labs such as Quest Diagnostics. Many OB‑GYN practices coordinate the collection on‑site. If you prefer a home‑based approach, order an at‑home kit online; the sample is mailed to a certified lab for analysis. Primary‑care physicians can also order comprehensive male work‑ups, including hormone panels and scrotal ultrasounds. testing is assess after 12 months of trying to conceive (or 6 months when either partner is over 35).
 Where can I get a fertility test done (female) You can schedule a comprehensive fertility work‑up at a women‑focused OB/GYN or reproductive endocrinology practice in Queens, NY. These clinics offer on‑site blood panels (AMH, FSH, estradiol, progesterone, thyroid, prolactin) and transvaginal ultrasound for ovarian reserve and uterine anatomy. For a convenient at‑home option, Labcorp OnDemand provides a Women’s Fertility Ovarian Reserve Test that can be completed at any certified collection site or pharmacy. Walgreens and other pharmacy chains also stock at‑home hormone kits that can be mailed for analysis. If imaging is needed, a hysterosalpingogram (HSG) or sonohysterogram can be arranged through the same specialist.
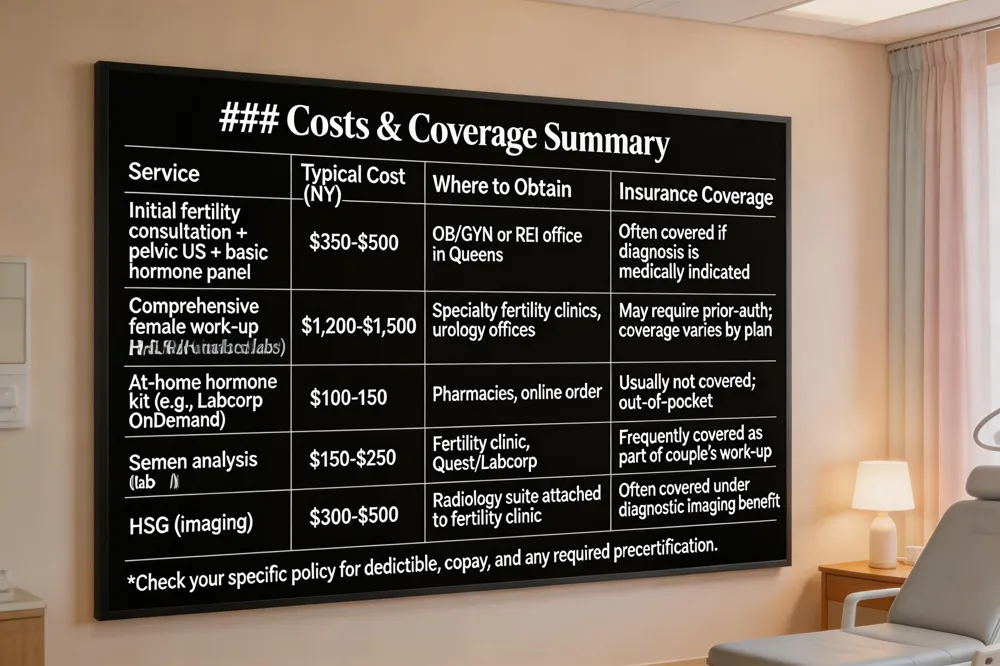
Fertility evaluation cost Initial consultations that include a pelvic ultrasound and basic hormone testing typically range from $350 to $500 in New York. More extensive packages that add multiple monitoring visits, advanced imaging, or male partner testing can cost $1,200–$1,500. Prices vary by provider, test complexity, and whether additional procedures (e.g., HSG) are required. Most offices have financial counselors to provide personalized estimates and discuss payment plans.
Is fertility evaluation covered by insurance? In states with infertility‑insurance mandates, a diagnostic fertility evaluation is usually a covered benefit, though coverage details differ by plan. Major carriers such as Aetna, BlueCross BlueShield, and Cigna often reimburse the evaluation portion even where a mandate does not exist, while more expensive treatments like IVF may be limited. Self‑insured employers and some small‑group plans may be exempt. Verify your policy and obtain any required precertification from your provider to ensure reimbursement.
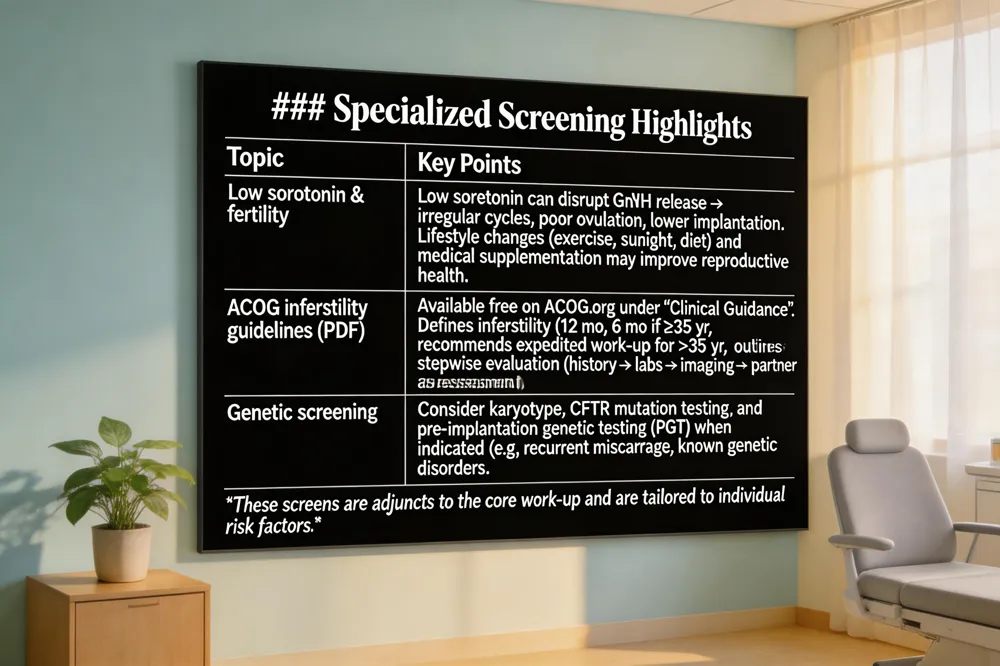 Can low serotonin cause infertility? Low serotonin levels are associated with mood disorders such as depression and anxiety, which can disrupt the hormonal balance required for normal reproductive function. Serotonin influences the release of gonadotropin‑releasing hormone (GnRH), a key driver of the menstrual cycle, ovulation and luteal phase. When serotonin is deficient, GnRH secretion may become irregular, potentially leading to irregular cycles, poor ovulation and lower implantation rates, all of which can reduce fertility. Although low serotonin is usually one of many contributing factors, improving serotonin through diet, exercise, stress management, sunlight exposure, adequate sleep, or medically guided supplementation can support reproductive health as part of a comprehensive fertility plan.
Infertility Guidelines ACOG pdf The American College of Obstetricians and Gynecologists (ACOG) makes its infertility guidelines freely available as a downloadable PDF on the ACOG website. Visit acog.org, select “Clinical Guidance” or “Practice Bulletins,” and search for “Infertility” or the specific bulletin number (e.g., Practice Bulletin 104, updated 2019). The PDF includes definitions, evaluation recommendations, and treatment options for both female and male factors, as well as age‑specific counseling. Use the site’s search bar with the keywords “Infertility Guidelines PDF” to locate the exact download page.
ACOG infertility guidelines ACOG defines infertility as the inability to achieve pregnancy after 12 months of regular, unprotected intercourse (or 6 months for women > 35 years). The College recommends an expedited evaluation after 6 months for women > 35 years and immediate evaluation for women > 40 years. Anticipatory counseling about the natural decline in ovarian reserve should be offered early, emphasizing realistic expectations and evidence‑based family‑building options. Evaluation includes a detailed history, hormonal testing, imaging, and partner assessment, with treatment ranging from lifestyle modification to assisted reproductive technologies. ACOG stresses clear, personalized patient education to counter misinformation.
 A thorough fertility evaluation begins after 12 months of regular, unprotected intercourse (or 6 months if the woman is over 35) and includes a detailed reproductive history, physical exam, and Baseline blood tests (FSH, LH, AMH, estradiol, progesterone, prolactin, thyroid) on specific cycle days. Transvaginal ultrasound for uterine anatomy, ovarian size, and antral follicle count assesses uterine anatomy and antral follicle count, while HSG or SHG imaging to assess tubal patency and intrauterine abnormalities confirms tubal patency. The male partner undergoes a Semen analysis after 2‑5 days abstinence for count, motility, morphology, volume, and pH, with Advanced male testing (e.g., sperm DNA fragmentation) when standard parameters are borderline.
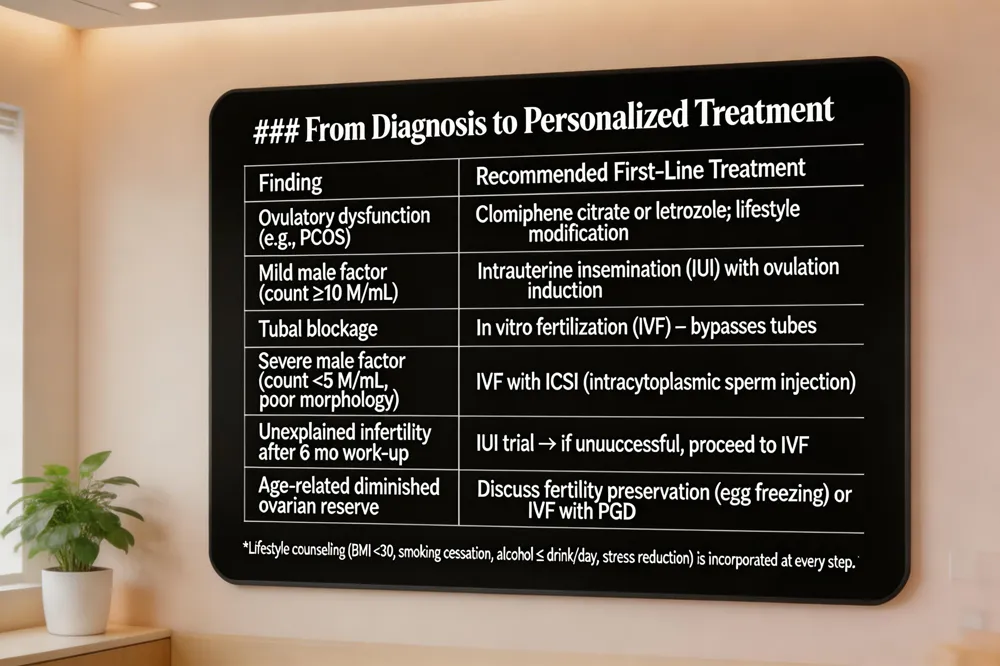
Personalized treatment options are built on these findings. Ovulation disorders may be managed with clomiphene citrate or letrozole; mild male factor or unexplained infertility often responds to intrauterine insemination (IUI); tubal blockage, severe male factor, or failed IUI typically leads to in‑vitro fertilization (IVF) with or without pre‑implantation genetic testing.
Lifestyle counseling (nutrition, weight management, smoking cessation, alcohol moderation, stress reduction) is a cornerstone of care. Couples are advised to achieve a healthy BMI (<30 kg/m²), quit smoking, limit alcohol and caffeine, optimize nutrition, and reduce stress—interventions that can improve ovulation, sperm quality, and ART outcomes.
Future planning and assisted technologies include fertility preservation (egg or sperm freezing) for those wishing to delay childbearing, and discussion of donor gametes or gestational carriers when indicated. Our woman‑led, Queens‑based practice integrates these evidence‑based strategies with compassionate, individualized guidance, ensuring each couple a clear roadmap from diagnosis to the most appropriate treatment pathway.
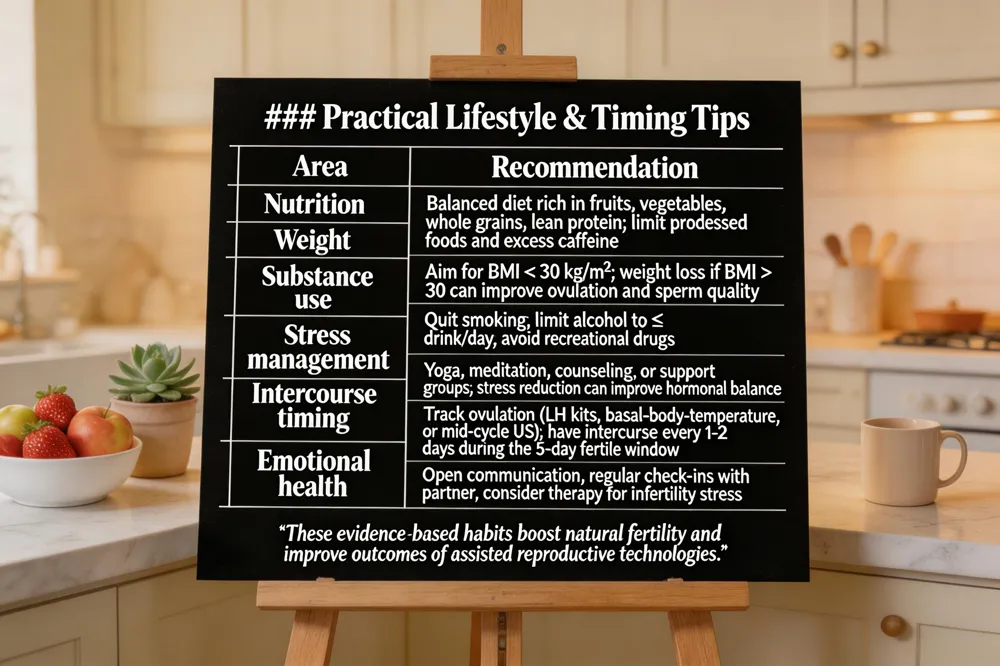 A healthy lifestyle sets the foundation for fertility. Aim for a balanced diet rich in fruits, vegetables, whole grains, and lean protein, maintain a BMI below 30 kg/m², quit smoking, limit alcohol to ≤ 1 drink per day, and manage stress through yoga, meditation, or counseling. Timely intercourse maximizes chances of conception: track ovulation with luteinizing‑hormone kits, basal‑body‑temperature charts, or a mid‑cycle transvaginal ultrasound, and have intercourse every 1‑2 days during the fertile window (the five days before and the day of ovulation). Emotional well‑being is equally vital—regularly discuss hopes and concerns with each other, seek support groups or a therapist experienced in infertility, and consider pre‑conception counseling to address anxiety, grief, or relationship strain. Together, these lifestyle, timing, and emotional strategies empower couples to move forward confidently while awaiting pregnancy.
By now you’ve learned the nine essential steps of a comprehensive fertility work‑up: (1) a detailed reproductive and medical history, (2) baseline hormone blood tests timed to the menstrual cycle, (3) transvaginal ultrasound with antral follicle count, (4) semen analysis for the male partner, (5) hysterosalpingography or sonohysterography to confirm tubal patency, (6) genetic or chromosomal screening when indicated, (7) lifestyle and environmental risk assessment, (8) a joint review of all findings, and (9) a personalized treatment plan that may include medication, IUI, IVF, or surgery.
If any of these steps feel overwhelming, know that you do not have to navigate them alone. Our compassionate team at the Queens Fertility Center is ready to guide you through each stage, answer your questions, and tailor a plan that respects your goals and circumstances.
Take the next step toward your family‑building journey—call us today at (212) 555‑1234 or visit www.queensfertilityclinic.com to schedule a confidential consultation. Your path to parenthood begins with a single, supportive conversation.
.png)
Compassionate care for every stage of womanhood. Visit one of our convenient locations or book your appointment online today.

